Many parents might be surprised to learn that diabetes in children is more common than they think — and it’s becoming more frequent. Every day across the United States, children are diagnosed with both Type 1 and Type 2 diabetes. From 2001 to 2017, the number of young people with Type 1 diabetes increased by 45%, and those with Type 2 by 95%. Catching the signs early can make a world of difference: when a child is diagnosed and begins treatment promptly, they have the best chance to lead a full and active life. This guide explains what to watch for, how diagnoses occur, what current treatments involve, and helpful ways to support your child both at home and at school.
Jump to: Frequently Asked Questions
📋 Quick Reference: Diabetes in Children
- Warning signs: Excessive thirst, frequent urination, unexplained weight loss, and extreme fatigue are the most common early signs of Type 1. Type 2 may cause fewer obvious symptoms initially.
- DKA is a medical emergency: Fruity-smelling breath, vomiting, or stomach pain in a child with suspected diabetes means go to the emergency room — not urgent care, not a next-day appointment.
- Both types are rising: Type 1 diabetes in U.S. youth increased 45% and Type 2 increased 95% between 2001 and 2017.
- Technology has transformed care: CGMs and automated insulin delivery (AID) systems are now recommended by the ADA for children with Type 1 diabetes.
- School planning is essential: Children with diabetes need legal accommodations and a written medical care plan to stay safe during the school day.
What are the two types of diabetes in children?
Both Type 1 and Type 2 diabetes can be diagnosed in children, though they differ in what causes them, how they appear, and how they are treated. Knowing the type your child has is an important first step for everything that comes next.
| Type 1 Diabetes in Children | Type 2 Diabetes in Children |
|---|---|
| Autoimmune condition — the body attacks insulin-producing cells in the pancreas | The body becomes resistant to insulin, or doesn’t produce enough to compensate |
| Can occur at any age; most common in childhood and adolescence | Historically seen in adults; now rising rapidly in children, especially teens |
| Requires insulin therapy for life — there is no alternative | Can often be managed with lifestyle changes; may require metformin or insulin |
| Weight is not a primary risk factor | Strongly associated with overweight, obesity, and sedentary lifestyle |
| Onset is often rapid — symptoms appear suddenly over days to weeks | Onset is often gradual; symptoms may be subtle or absent for a long time |
Important: In children and teens, the type of diabetes is not always clear at diagnosis. Some children with Type 1 may also have overweight or insulin resistance, and some children with Type 2 may present with ketosis. Autoantibody and C-peptide testing help clarify the diagnosis and should be part of the workup when the type is uncertain.
What are the early signs of diabetes in children?

Detecting diabetes early — before it turns into a serious issue — is one of the most important steps parents and caregivers can take. The signs of Type 1 usually appear suddenly and can worsen quickly, so recognizing them early can make a real difference.
Symptoms of Type 1 diabetes
- Excessive thirst: Your child is drinking much more than usual and is never satisfied.
- Frequent urination: Trips to the bathroom every hour or two, including at night. Previously toilet-trained young children may have accidents again.
- Unexplained weight loss: Without insulin, the body breaks down fat and muscle for energy instead.
- Extreme hunger: Because glucose can’t enter cells, the body signals constant hunger even after eating.
- Fatigue and weakness: Cells starved of glucose produce an exhaustion that’s different from normal tiredness.
- Blurred vision: High blood sugar causes fluid shifts in the eye’s lens, temporarily blurring vision.
- Fruity-smelling breath, nausea, vomiting, or stomach pain: These symptoms together may indicate diabetic ketoacidosis (DKA) — a life-threatening emergency. Go to the emergency department immediately.
Symptoms of Type 2 diabetes
Type 2 in children may initially have no obvious symptoms. When symptoms do appear, they can include:
- Increased thirst and frequent urination
- Fatigue and sluggishness
- Dark, velvety patches of skin (acanthosis nigricans): Found on the back of the neck, armpits, or groin — a visible sign of insulin resistance.
- Slow-healing cuts or wounds
- Blurry vision
If your child shows signs such as excessive thirst, frequent urination, and weight loss, contact your doctor the same day. For symptoms such as fruity-smelling breath, vomiting, stomach pain, or confusion, go directly to the emergency room. Don’t wait for an appointment or visit urgent care — DKA can become life-threatening within hours.
What puts a child at risk for diabetes?
| Type 1 Diabetes Risk Factors | Type 2 Diabetes Risk Factors |
|---|---|
| Family history of Type 1 diabetes | Overweight or obesity, especially abdominal weight |
| Having a sibling with Type 1 increases risk significantly | Family history of Type 2 diabetes in a parent or sibling |
| Other autoimmune conditions (celiac disease, thyroid disease) | Sedentary lifestyle; less than 60 minutes of physical activity most days |
| Viral infections may trigger the autoimmune response in predisposed children | Higher rates in Black, Hispanic, Asian American, and American Indian youth |
| Diabetes-related autoantibodies (screenable before symptoms appear) | Previous diagnosis of prediabetes |
New research suggests that COVID-19 infection may also increase the risk of Type 2 diabetes in some children, though the magnitude and mechanisms remain under study. The TEDDY study (Environmental Determinants of Diabetes in the Young) has shown that viral infections and other environmental triggers may contribute to Type 1 diabetes in genetically predisposed children. The ADA 2026 Standards now recommend offering autoantibody screening to children with a family history of Type 1 diabetes or a known elevated genetic risk.
How is diabetes diagnosed in children?
Diabetes is diagnosed with blood tests. If your child shows symptoms, a same-day test is appropriate — Type 1 diabetes can progress to DKA within hours.
- Fasting blood sugar test: A result of 126 mg/dL (7.0 mmol/L) or higher after an overnight fast indicates diabetes.
- Random blood sugar test: A result of 200 mg/dL (11.1 mmol/L) or higher at any time, along with symptoms, confirms diabetes.
- A1c test: A result of 6.5% or higher indicates diabetes. A result between 5.7% and 6.4% indicates prediabetes. See the A1c overview for how this test works.
- Autoantibody testing: If Type 1 is suspected, autoantibody tests (GAD, IA-2, ZnT8, insulin autoantibodies) help confirm the autoimmune diagnosis.
- C-peptide test: Measures how much insulin the pancreas is still producing. Helps differentiate Type 1 from Type 2, especially when the type is unclear at diagnosis.
How is diabetes treated in children?
Treatment for diabetes in children has improved dramatically over the past decade. Today’s care is much more effective than it was even five years ago.
Type 1 diabetes treatment
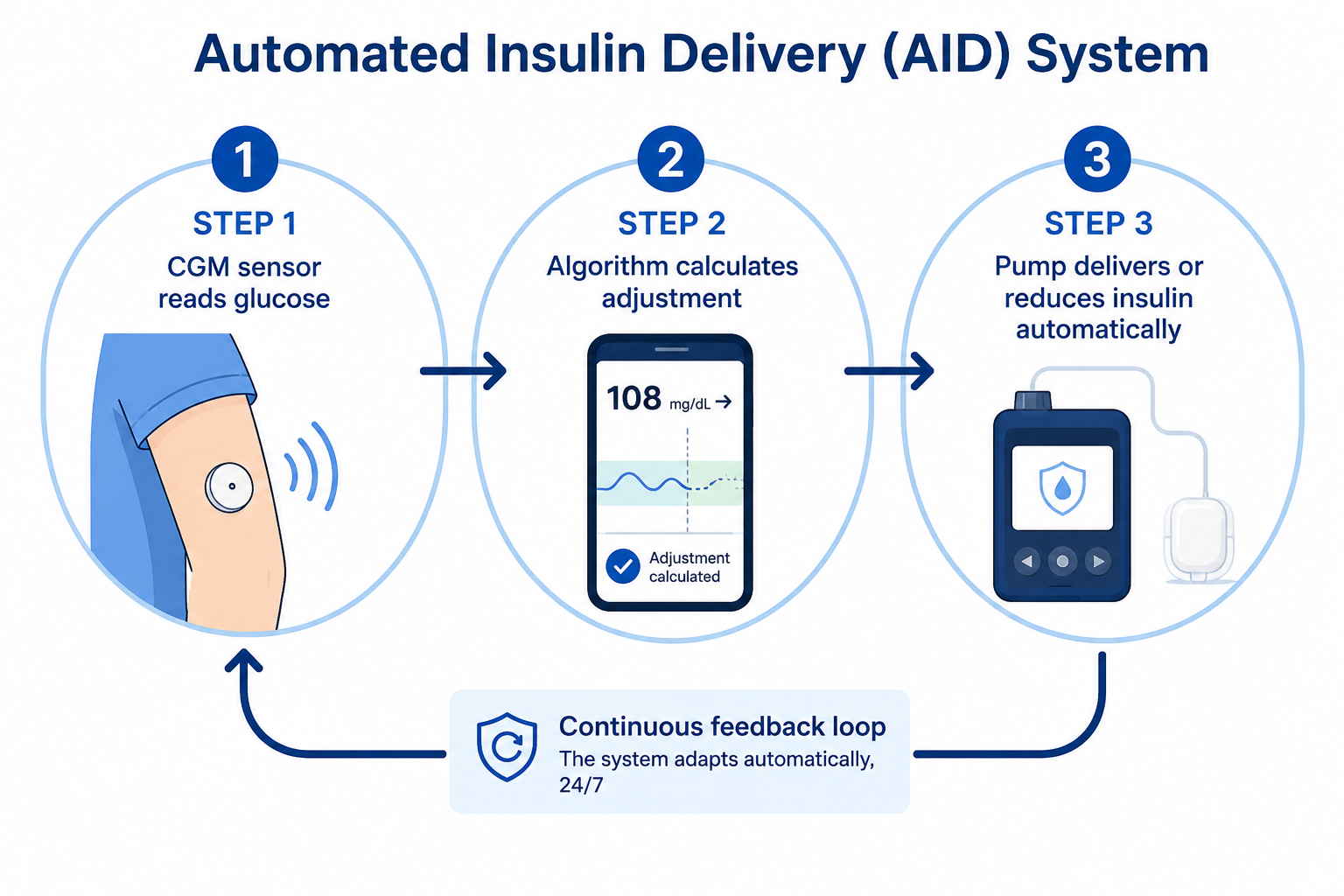
Children with Type 1 diabetes require insulin to survive. Today, the most effective approach combines a continuous glucose monitor (CGM) with an automated insulin delivery (AID) system.
- Automated insulin delivery (AID) systems: The ADA 2026 Standards recommend AID systems for all children with Type 1 diabetes who can use them safely. These systems integrate a CGM with an insulin pump that automatically adjusts insulin delivery based on real-time glucose readings, reducing both high and low blood sugar and easing the management burden for children and families.
- Continuous glucose monitors (CGMs): The ADA recommends offering CGMs to children with Type 1 at diagnosis or as soon as possible. CGMs track glucose continuously and alert parents and children to trends before they become dangerous.
- Multiple daily injections (MDI): For families who cannot access a pump or prefer not to use one, multiple daily injections of long-acting and short-acting insulin remain effective, especially when used with a CGM.
- Carbohydrate counting: Matching insulin to carbohydrate intake is a foundational skill. See the carbohydrate counting guide for practical guidance.
A1c goals for children with Type 1: The ADA recommends an A1c below 7% for most children, with individualized goals based on age and hypoglycemia risk.
Type 2 diabetes treatment in children
- Healthy nutrition and weight management: The foundation of Type 2 management. Reducing sugar-sweetened beverages, increasing vegetable intake, and limiting processed foods can significantly improve insulin sensitivity.
- Physical activity: At least 60 minutes of moderate-to-vigorous activity daily is recommended.
- Metformin: The first-line medication for most children with Type 2 diabetes. It improves insulin sensitivity and is generally well-tolerated.
- Insulin: Children with very high blood sugar, DKA, or those who don’t respond to oral medications may need insulin, at least initially.
A1c goals for children with Type 2: The ADA recommends an A1c below 6.5% for most children with Type 2 — a tighter target because the risk of low blood sugar is lower in Type 2 management.
Ketone testing — what families should know
Families should have ketone strips or a blood ketone meter at home and know when to use them. Check for ketones during illness, persistent vomiting, any blood sugar reading above 250 mg/dL (13.9 mmol/L) that doesn’t come down with correction, or suspected pump failure. Ketones building up in the blood is the first step toward DKA — early detection allows intervention before a hospital visit becomes necessary. Ask your care team what ketone level warrants emergency care.
Growth — what families should know
Children grow and become adults. With each growth spurt, a child needs more insulin. This is normal and does no harm to the child. The extra insulin helps regulate blood sugar, an essential part of staying healthy throughout childhood and adolescence.
How do I manage my child’s diabetes at school?
School is one of the most important — and logistically challenging — settings for a child with diabetes. Without proper planning, diabetes can disrupt learning, physical activity, and social life.
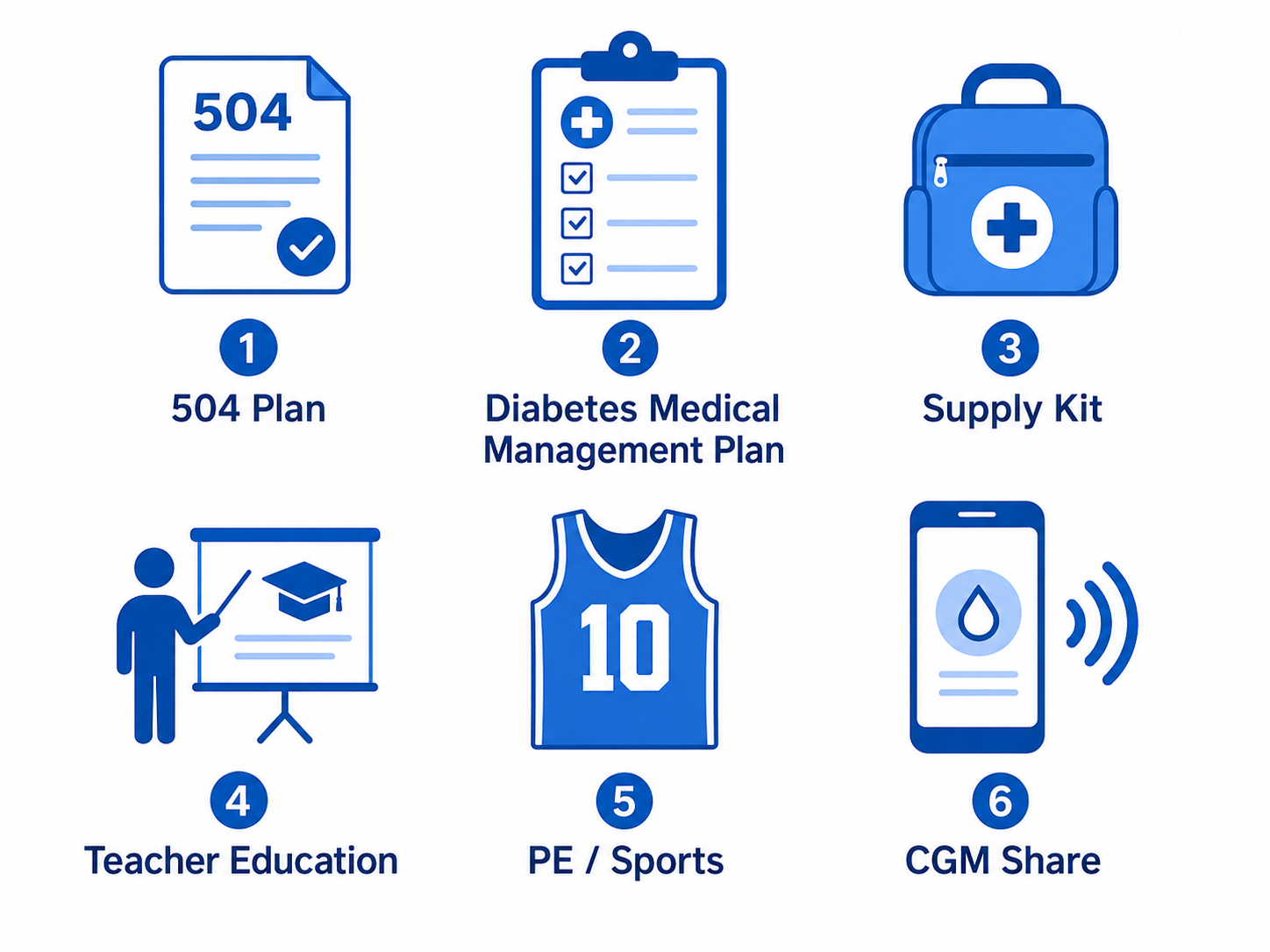
- Understand the difference between a 504 Plan and an Individual Health Plan (IHP): A 504 Plan is a civil-rights accommodation plan that protects your child’s access to school activities and accommodations (such as the right to check blood sugar in class or to eat a snack at any time). An Individual Health Plan (IHP) or Diabetes Medical Management Plan (DMMP) outlines day-to-day medical care — insulin doses, when to call parents, how to treat lows, and so on. Many children need both. Work with your school nurse, care team, and administrator to put both in place.
- Educate key staff: Teachers, coaches, and the school nurse should know the symptoms of low blood sugar, how to use glucagon if your child has it, and what to do in an emergency.
- Keep supplies at school: A supply kit containing glucose tablets, juice, a backup meter and strips, and glucagon should be kept in the nurse’s office. Older children should carry a personal kit.
- Address exercise: The ADA 2026 Standards recommend a pre-exercise blood sugar target of 126–180 mg/dL (7.0–10.0 mmol/L) for children. Communicate your child’s specific plan to PE teachers and coaches.
- CGM sharing: Many CGM systems enable remote monitoring via a smartphone app, allowing parents to receive out-of-range alerts during the school day.
How can I support my child emotionally with diabetes?
A diabetes diagnosis can significantly impact family life, bringing new daily challenges with monitoring, insulin management, and planning. The ADA 2026 Standards highlight the importance of behavioral health professionals in pediatric diabetes care — annual behavioral health screening is now recommended for all children with diabetes.
- Normalize the condition: Children take cues from adults. The calmer diabetes is managed, the less frightening it becomes.
- Watch for diabetes distress and burnout: Feeling overwhelmed, angry, or hopeless about diabetes is common among children and teens — and among parents. Both deserve attention.
- Connect with other families: Diabetes camps, family support groups, and online communities help children realize they’re not alone.
- Gradually transfer responsibility: As children grow, the goal is to increase self-management. Pushing too fast leads to errors; moving too slowly prevents independence.
⚠️ Medical disclaimer: This article is for educational purposes and does not replace medical care. If your child shows signs of diabetic ketoacidosis — fruity-smelling breath, vomiting, confusion, or severe stomach pain — go to the emergency room immediately. Always work with your child’s diabetes care team for individualized management decisions.
Helpful Resources & Research
- ADA Standards of Care 2026: Section 14 — Children and Adolescents
- JDRF (Juvenile Diabetes Research Foundation)
- Children with Diabetes
- Diabetes Camping Association
- KidsHealth: Managing Diabetes
- ADA: Resources for Parents and Kids
- NCBI: Diabetes in Children and Adolescents — Diabetes in America (December 2025)
Frequently Asked Questions — Diabetes in Children
What are the early signs of diabetes in a child?
The most common early signs of Type 1 diabetes include excessive thirst, frequent urination (including nighttime accidents in previously toilet-trained children), unexplained weight loss, and unusual fatigue. Fruity-smelling breath, nausea, vomiting, or stomach pain together are signs of diabetic ketoacidosis — go to the emergency room immediately if you see these. For Type 2, symptoms may be subtler, including dark skin patches (acanthosis nigricans), fatigue, and slow-healing wounds.
How does Type 1 diabetes differ from Type 2 diabetes in children?
Type 1 is an autoimmune disease in which the body destroys insulin-producing cells. It currently requires lifelong insulin and is not caused by diet or weight. Type 2 develops when the body becomes insulin-resistant and is more common in overweight children. In practice, the types are not always obvious at diagnosis — autoantibody and C-peptide testing help clarify the diagnosis when there is uncertainty.
Can a child with Type 1 diabetes use an insulin pump?
Yes—the ADA 2026 Standards recommend automated insulin delivery (AID) systems for all children with Type 1 who can use them safely. These systems pair a CGM with a pump that automatically adjusts insulin based on real-time glucose levels, helping reduce both high and low blood sugar. They can be used even in very young children when parents manage the device.
What A1c should my child aim for?
The ADA recommends an A1c below 7% for most children with Type 1 diabetes, with individualized goals based on age, hypoglycemia risk, and other factors. For children with Type 2 diabetes, the target is below 6.5%. Your care team will determine the most appropriate target for your child.
What is the difference between a 504 Plan and a diabetes health plan in school?
A 504 Plan is a civil-rights accommodation plan that protects your child’s access to school activities — such as the right to check blood sugar in class or to eat a snack at any time. An Individual Health Plan or Diabetes Medical Management Plan (DMMP) outlines day-to-day medical care: insulin doses, how to treat lows, when to call parents, and more. Most children with diabetes need both. Work with the school nurse, administrator, and your care team to put both documents in place before the school year begins.
Can my child with diabetes play sports?
Absolutely. Exercise requires extra planning — blood sugar often drops during and after physical activity, so snacks and dose adjustments may be needed. The ADA recommends a pre-exercise blood sugar target of 126–180 mg/dL (7.0–10.0 mmol/L) for children. Talk to your care team about a specific exercise plan, and ensure coaches know the signs of low blood sugar.
What is DKA, and how can I prevent it?
Diabetic ketoacidosis (DKA) is a life-threatening condition that occurs when the body lacks insulin and begins producing acidic ketones as it burns fat. Symptoms include fruity-smelling breath, nausea, vomiting, stomach pain, and altered consciousness. Families should keep ketone strips or a blood ketone meter at home and know when to test: during illness, with persistent high blood sugar, or when pump failure is suspected. Consistent insulin use and regular monitoring are the best prevention.
Will my child outgrow their diabetes?
No. Type 1 diabetes is a lifelong condition. Children with Type 1 do not outgrow it, and their insulin needs will change as they grow, go through puberty, and eventually manage their own care. Type 2 diabetes can sometimes improve significantly with weight loss and lifestyle changes, but it should still be monitored throughout life.
Are there diabetes camps for children?
Yes, they can be transformative. Diabetes camps offer children the experience of a typical summer camp, surrounded by peers who understand what they’re going through, with medical staff on hand. The Diabetes Camping Association maintains a worldwide directory at diabetescamps.org.
How can I help prevent my child from developing Type 2 diabetes?
The strongest protective factors include maintaining a healthy weight, eating a balanced diet low in added sugars and processed foods, and staying physically active for at least 60 minutes on most days. If your child has prediabetes or risk factors for Type 2, ask your doctor about formal diabetes prevention programs, which have strong evidence of effectiveness in both adults and adolescents.
Last Updated on June 2, 2026