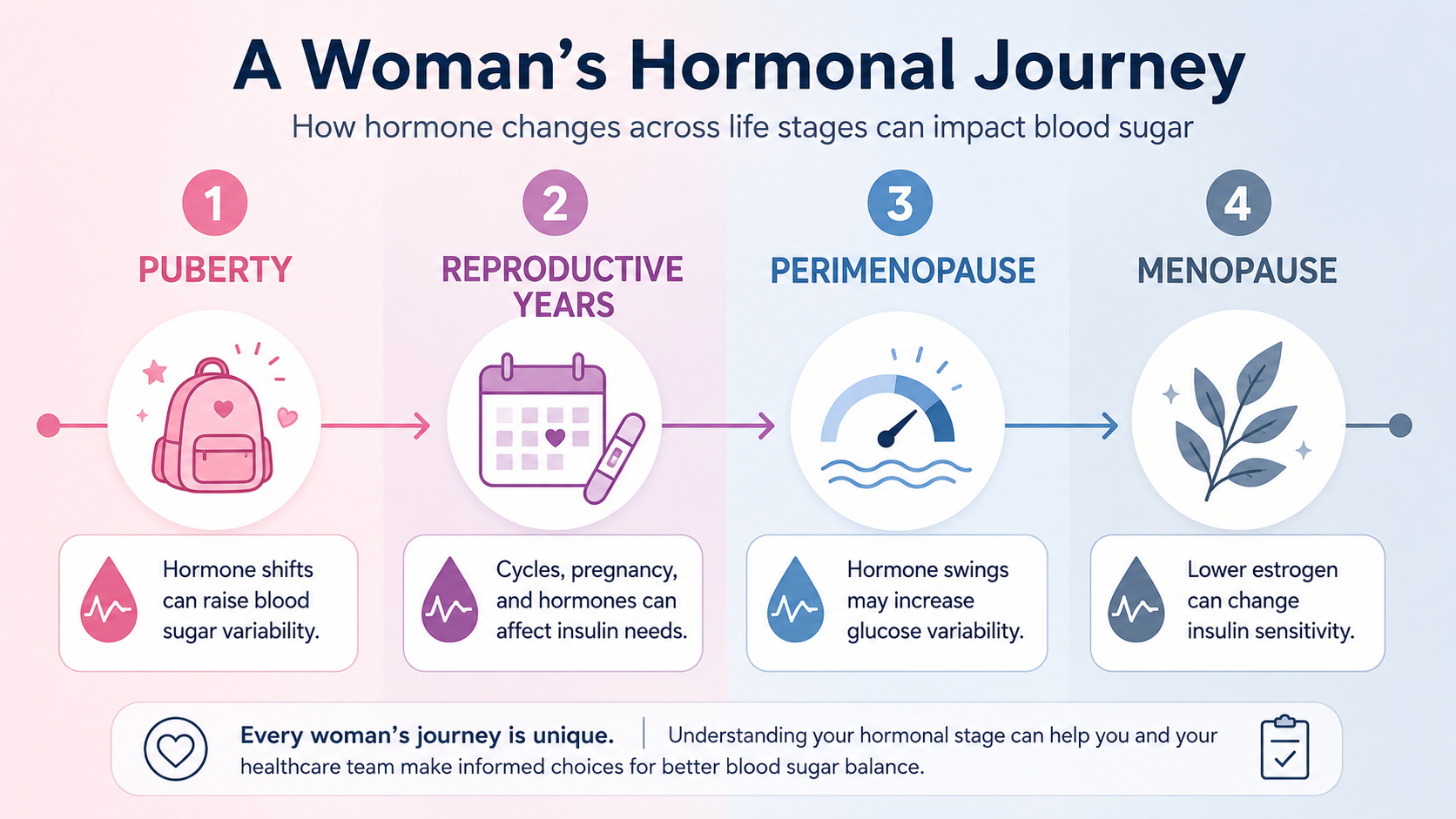
Women with diabetes face a unique set of challenges that are all their own. Hormonal changes throughout life — from the first menstrual cycle through pregnancy and menopause — can significantly shift blood sugar levels in ways that are hard to predict without the right knowledge. This guide covers the key life stages where hormones and diabetes intersect, what the latest research recommends, and practical strategies you can use at every phase.
Jump to: Frequently Asked Questions
📋 Quick Summary: How Hormones Affect Blood Sugar in Women
- Menstrual cycle: Progesterone in the second half of your cycle often raises blood sugar 3–5 days before your period.
- PCOS: Polycystic ovary syndrome is strongly linked to insulin resistance and raises the risk of type 2 diabetes.
- Pregnancy: Tight blood sugar control is critical before and throughout pregnancy. Many medications must be stopped before conceiving.
- Menopause: Falling estrogen increases insulin resistance and makes blood sugar harder to predict.
- Key tool: A CGM is especially valuable for women with diabetes — hormonal patterns are visible in the data long before you feel them.
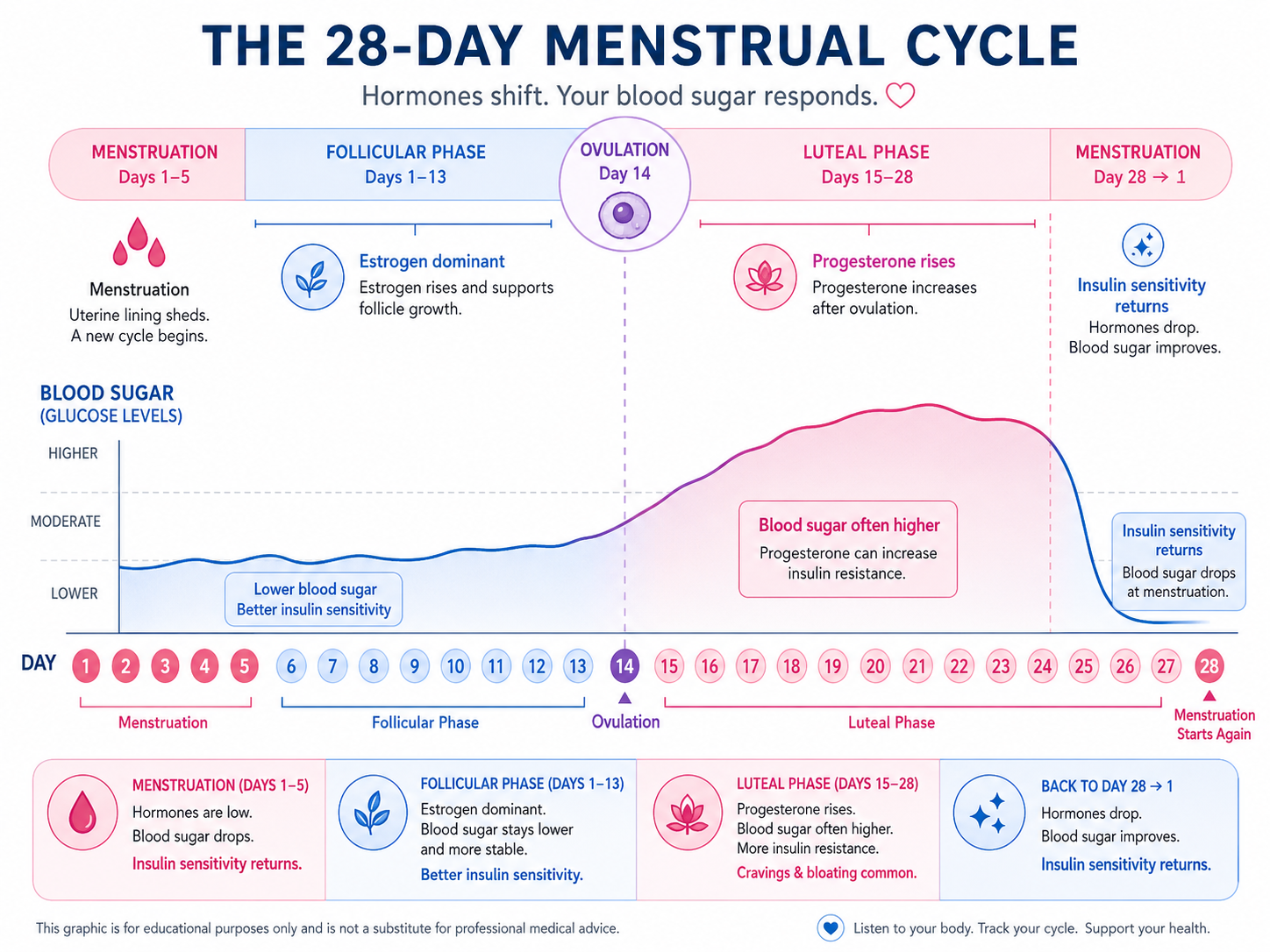
How does the menstrual cycle affect blood sugar levels?
Your menstrual cycle is driven by rising and falling levels of estrogen and progesterone. Both hormones influence how your body responds to insulin — and they don’t always cooperate.
During the luteal phase (the second half of your cycle, after ovulation), progesterone levels rise. This hormone reduces insulin sensitivity, meaning your cells don’t respond to insulin as efficiently as usual. For many women with diabetes, this translates to higher blood sugar for 3–5 days before menstruation begins — sometimes requiring a temporary increase in insulin or medication.
After your period starts, progesterone drops and insulin sensitivity typically returns. This shift can cause blood sugar to fall, sometimes quickly. Tracking your cycle alongside your glucose data helps you anticipate these swings and respond proactively rather than reactively.
Practical tips for the menstrual cycle
- Monitor more frequently: In the week before your period, check your blood sugar more often — or make sure your CGM alerts are set and active.
- Track your cycle alongside glucose data: Use a period-tracking app alongside your glucose readings. After 2–3 months, patterns become clear enough to plan ahead.
- Adjust if needed — with guidance: Some women need a temporary insulin increase in the days before their period. Discuss this with your care team rather than adjusting on your own.
- Stay active: Even gentle walking during PMS can improve insulin sensitivity and reduce blood sugar fluctuations.
- Watch cravings: High-protein, high-fiber snacks — such as Greek yogurt with berries or nuts with a small piece of dark chocolate — are easier on blood sugar than high-carb comfort foods.
Polycystic ovary syndrome (PCOS) affects approximately 6–10% of women of reproductive age and is one of the most common hormonal conditions in women with diabetes or prediabetes. At its core, PCOS is driven by insulin resistance — the same mechanism that underlies Type 2 diabetes.
Common signs of PCOS
- Irregular, infrequent, or absent periods
- Excess facial or body hair (hirsutism)
- Acne, particularly along the jawline
- Weight gain, especially around the abdomen, or difficulty losing weight
- Difficulty becoming pregnant
- Dark, velvety patches of skin (acanthosis nigricans) — a sign of insulin resistance
Not all women with PCOS have all of these symptoms, and many are diagnosed only when they have trouble conceiving. If you have Type 2 diabetes or prediabetes and irregular periods, ask your doctor about PCOS screening.
Managing PCOS and diabetes together
| Approach | How It Helps |
|---|---|
| Metformin | Improves insulin sensitivity and may help regulate cycles in women with PCOS |
| GLP-1 receptor agonists / dual incretin medications | Support weight loss and reduce insulin resistance; increasingly used in PCOS management, but must be stopped before pregnancy |
| Regular exercise | Resistance training and aerobic activity both improve insulin sensitivity |
| Low-glycemic eating | Reduces glucose spikes and insulin demand, which can help ease PCOS symptoms |
| Hormonal contraceptives | Can regulate cycles and reduce androgen symptoms in women with PCOS who are not planning pregnancy |
How do I choose birth control if I have diabetes?
Most birth control methods are used safely by women with diabetes, but the right choice depends on your individual health profile — including your blood pressure, cardiovascular risk, history of blood clots, and whether you’re planning a pregnancy soon. This is a conversation to have with your care team, not a decision to make based on general lists.
- Progestin-only methods (hormonal IUDs, implants, the mini-pill) are often a good choice because they carry less cardiovascular risk than estrogen-containing options.
- Non-hormonal methods (copper IUDs, condoms, diaphragms) are appropriate for women who prefer to avoid hormones or who are at higher cardiovascular or clotting risk.
- Combined estrogen-progestin pills are used by many women with diabetes. If you use them, choose a low-dose estrogen formulation and monitor your blood pressure and cholesterol regularly.
- Long-acting reversible contraceptives (LARCs) — such as IUDs and implants — are among the most effective options and eliminate the need to remember a daily pill, which can matter when managing multiple aspects of diabetes care.
What do I need to know about pregnancy and diabetes?
Pregnancy is one of the most medically significant life events for a woman with diabetes, and planning ahead dramatically improves outcomes for both mother and baby. The ADA Standards of Care 2026 (Section 15) emphasizes that preconception counseling should begin well before a planned pregnancy — ideally months in advance.
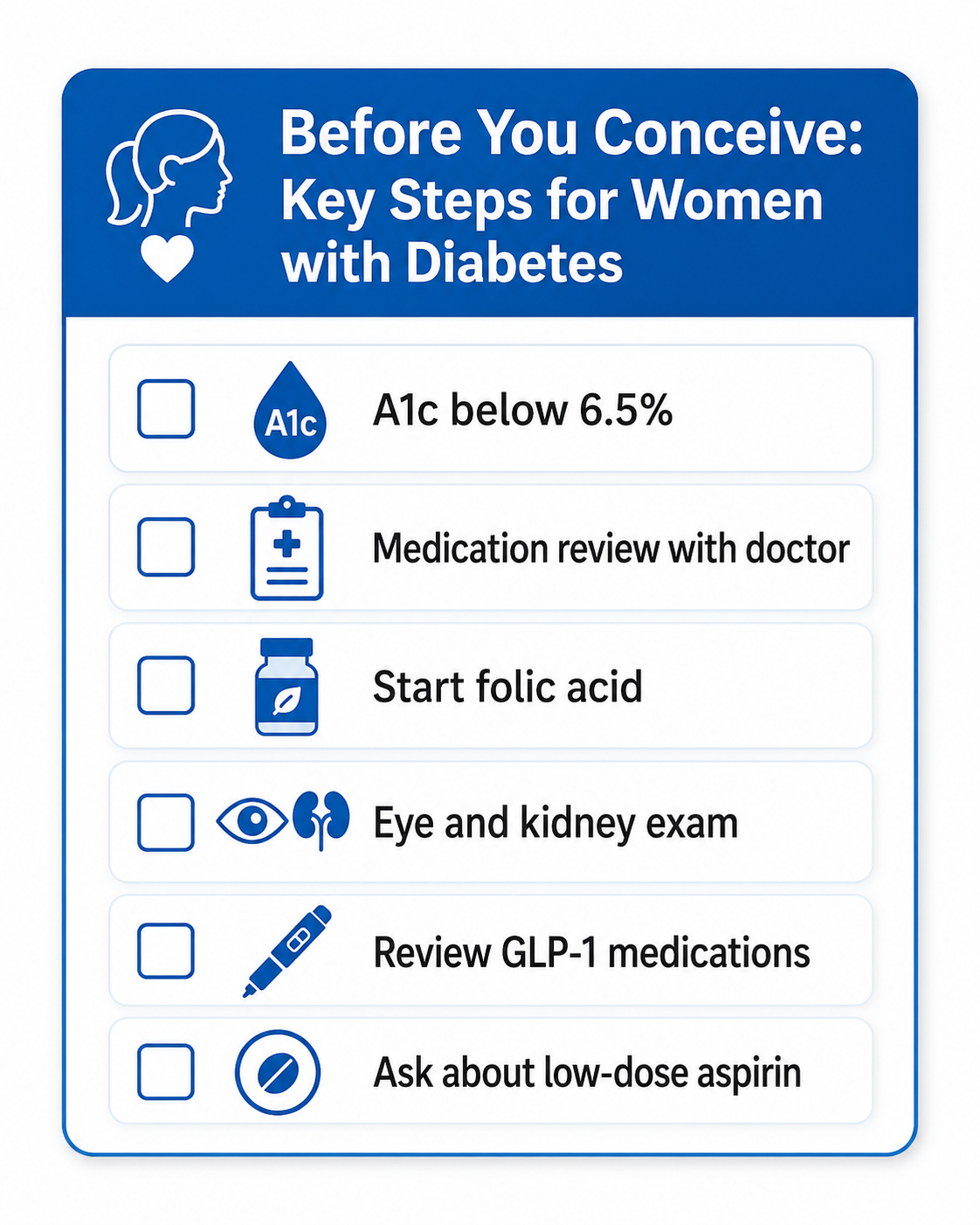
Before you conceive
- Blood sugar targets tighten significantly in pregnancy. The ADA recommends a target A1c below 6.5% before conception when this can be achieved safely. Even modest improvements before pregnancy reduce the risk of birth defects, miscarriage, and complications.
- Review GLP-1 and dual incretin medications well before pregnancy. Semaglutide is generally stopped at least 2 months before a planned pregnancy because of its long half-life. Tirzepatide timing should be individualized with your care team; some non-U.S. prescribing information recommends stopping at least 1 month before pregnancy. Do not stop suddenly without a replacement plan — rebound hyperglycemia or weight regain can also increase pregnancy risk.
- Review all medications. Several diabetes and blood pressure medications are not safe in pregnancy. Your care team will review your full medication list and make substitutions as needed.
- Start folic acid. 400–1,000 mcg daily is recommended for all women with diabetes planning pregnancy, as diabetes increases the baseline risk of neural tube defects.
- Get a full checkup. Eye exams, kidney function tests, and thyroid screening are all recommended before conception, as diabetes-related complications can worsen during pregnancy.
- Ask about low-dose aspirin. Women with preexisting diabetes are at increased risk for preeclampsia and other hypertensive disorders of pregnancy. Ask your care team whether low-dose aspirin is appropriate for you, as current guidelines recommend it for high-risk pregnancies.
During pregnancy
Blood sugar targets in pregnancy are more stringent than outside of pregnancy. The ADA recommends fasting glucose below 95 mg/dL (5.3 mmol/L) and 1-hour post-meal glucose below 140 mg/dL (7.8 mmol/L). A continuous glucose monitor (CGM) is strongly recommended during pregnancy to help you track these tight targets in real time.
For women using automated insulin delivery (AID) systems, the ADA 2026 Standards include specific counseling guidance for pregnancy, including when to switch between automated and manual modes. If you use an AID system and become pregnant, work with your care team to understand how to use it appropriately throughout each trimester.
Gestational diabetes — diabetes that develops for the first time during pregnancy — affects approximately 6–10% of pregnancies in the U.S. and is usually screened for between 24 and 28 weeks. It typically resolves after delivery, but increases the long-term risk of Type 2 diabetes for both mother and child.
After delivery
Insulin needs often fall quickly after delivery — sometimes dramatically — especially in women with Type 1 diabetes. Monitor your blood sugar levels closely in the days following birth and be prepared to adjust insulin doses as directed by your care team.
Women who have had gestational diabetes should receive postpartum diabetes screening, usually with a 75-gram oral glucose tolerance test at 4–12 weeks after delivery, and ongoing screening thereafter because of the significantly elevated lifetime risk of Type 2 diabetes.
How does menopause affect diabetes?
The transition to menopause — which typically begins in a woman’s mid-to-late 40s and can span several years — brings a significant drop in estrogen. Because estrogen supports insulin sensitivity, its decline makes blood sugar management more challenging. Many women find that the diabetes regimen that worked well for decades starts to feel unpredictable during perimenopause and menopause.
What changes during menopause
- Increased insulin resistance: Lower estrogen means your cells respond less efficiently to insulin. You may need medication adjustments.
- More variable blood sugar: Hot flashes, night sweats, and disrupted sleep all raise cortisol levels, which can push blood sugar up unexpectedly.
- Weight redistribution: Many women gain weight during menopause, particularly in the abdomen, which further increases insulin resistance.
- Hypoglycemia awareness may shift: Hot flashes and low blood sugar share some symptoms (sweating, heart pounding, feeling warm), which can make lows harder to recognize during menopause.
Hormone replacement therapy (HRT) and diabetes
HRT can improve menopause symptoms and may have modest benefits for insulin sensitivity. Transdermal estrogen (patch or gel) may carry a different clotting and metabolic risk profile than oral estrogen, though the evidence continues to evolve. The appropriateness of HRT depends heavily on your individual cardiovascular history, clotting risk, and personal preferences. Discuss the full picture with your gynecologist and diabetes care team together.
How does diabetes affect sexual health in women?
Sexual health complications from diabetes are common but rarely discussed openly. High blood sugar over time can affect nerve function and blood flow, which in turn affects sexual response and comfort. Good glucose management reduces — but does not always eliminate — these complications.
| Issue | What Helps |
|---|---|
| Vaginal dryness | Vaginal lubricants or moisturizers; ask your doctor about low-dose vaginal estrogen (local application, minimal systemic absorption) |
| Recurrent yeast infections | Keep blood sugar in range; consider probiotics; discuss antifungal options with your doctor |
| Painful intercourse | Pelvic floor physical therapy; vaginal estrogen if dryness is the cause; discuss vaginismus with your gynecologist |
| Low libido or difficulty reaching orgasm | May be hormonal, psychological, or neurological in origin; worth discussing with your care team as causes are often treatable |
⚠️ Medical disclaimer: This article is for educational purposes and does not replace medical care. For urgent symptoms such as vomiting, confusion, fruity-smelling breath, chest pain, or severe low blood sugar, seek emergency care immediately. Always discuss medication changes — including stopping GLP-1 medications or starting new treatments during pregnancy — with your care team.
Helpful Resources & Research
- ADA Standards of Care 2026: Section 15 — Management of Diabetes in Pregnancy
- American Diabetes Association: Women and Diabetes
- CDC: PCOS and Diabetes
- NICHD: PCOS Overview
- The Menstrual Cycle and Glucose Control (NIH, 2022)
- Cleveland Clinic: Menopause
Frequently Asked Questions — Women with Diabetes
Why does my blood sugar rise before my period?
Progesterone, which rises in the second half of your menstrual cycle, reduces your body’s insulin sensitivity. This makes it harder for your cells to take up glucose, raising blood sugar — often for 3–5 days before your period starts. Once menstruation begins and progesterone levels drop, insulin sensitivity typically returns, and blood sugar may fall.
Does PCOS increase my risk of developing diabetes?
Yes. PCOS is strongly linked to insulin resistance, the underlying driver of Type 2 diabetes. Women with PCOS have a significantly higher lifetime risk of developing both Type 2 and gestational diabetes. If you have PCOS, ask your doctor about regular blood sugar screening, even if you don’t yet have diabetes.
Can I get pregnant if I have diabetes?
Yes. Women with Type 1 and Type 2 diabetes have healthy pregnancies every day. The key is careful preparation: working with your care team to optimize blood sugar control before conception, reviewing all medications, and starting folic acid in advance. The ADA recommends a pre-pregnancy A1c below 6.5% when it can be safely achieved.
Do I have to stop my diabetes medications when trying to get pregnant?
Some medications need to be stopped or changed. Semaglutide is generally stopped at least 2 months before a planned pregnancy; tirzepatide timing should be individualized with your care team. Several blood pressure and other medications also require substitution. Talk to your care team well before you start trying to conceive, so you have a transition plan in place.
Can I use an insulin pump or CGM during pregnancy?
Yes, the ADA strongly recommends CGM use throughout pregnancy for women with diabetes. It helps you track the tighter blood sugar targets in real time. For pump and AID system users, the ADA 2026 Standards include specific guidance for pregnancy, including when to switch between automated and manual modes. Discuss your specific setup with your care team.
How does menopause affect diabetes management?
The drop in estrogen during menopause reduces insulin sensitivity, so your body needs more insulin to achieve the same effect. Many women find that blood sugar becomes more variable during perimenopause and menopause, and may need medication adjustments. Hot flashes and night sweats also raise cortisol, which can raise blood sugar. A CGM during this transition can help identify new patterns quickly.
Is hormone replacement therapy safe with diabetes?
HRT may modestly improve insulin sensitivity and help manage menopausal symptoms. Transdermal estrogen may carry a lower risk of clotting than oral estrogen, but all forms require individualized assessment. The decision depends on your cardiovascular health, clotting risk, and other factors. Discuss this with your gynecologist and diabetes care team.
Why do I keep getting yeast infections?
Yeast thrives on elevated blood sugar. Women with diabetes have a higher risk of recurrent vaginal yeast infections. Keeping your blood sugar in range is the most effective way to prevent them. If infections are frequent, your doctor can help determine whether blood sugar, antibiotic use, or other factors are contributing.
Can diabetes affect sexual function in women?
Yes. High blood sugar over time can affect nerve function and blood flow, leading to reduced sensation, vaginal dryness, and difficulty reaching orgasm. Treatments are available for most of these issues — speak openly with your care team, as these problems are more common than reported.
What blood sugar targets should I aim for during pregnancy?
Targets during pregnancy are tighter than those outside of pregnancy. The ADA recommends fasting blood sugar below 95 mg/dL (5.3 mmol/L) and 1-hour post-meal blood sugar below 140 mg/dL (7.8 mmol/L). These goals reduce the risk of complications for you and your baby. A CGM makes tracking these targets throughout the day much easier.
Last Updated on June 2, 2026