 If you have been newly diagnosed with diabetes, the first thing to know is this: millions of people live well with diabetes every day. A diagnosis brings a rush of new terms, decisions, and adjustments all at once — but you do not have to figure it out alone or all at once. This guide is your starting point. It walks you through the most important topics in the order that makes sense, so you know what to tackle first and where to go for deeper information.
If you have been newly diagnosed with diabetes, the first thing to know is this: millions of people live well with diabetes every day. A diagnosis brings a rush of new terms, decisions, and adjustments all at once — but you do not have to figure it out alone or all at once. This guide is your starting point. It walks you through the most important topics in the order that makes sense, so you know what to tackle first and where to go for deeper information.
Each section below links to a dedicated article in our Newly Diagnosed series, written specifically for people who are early in their diabetes journey. You can read them from beginning to end or jump directly to the topic you need most right now. Either way, you are in the right place.
Searching for a specific answer? Jump to our Frequently Asked Questions for quick answers.
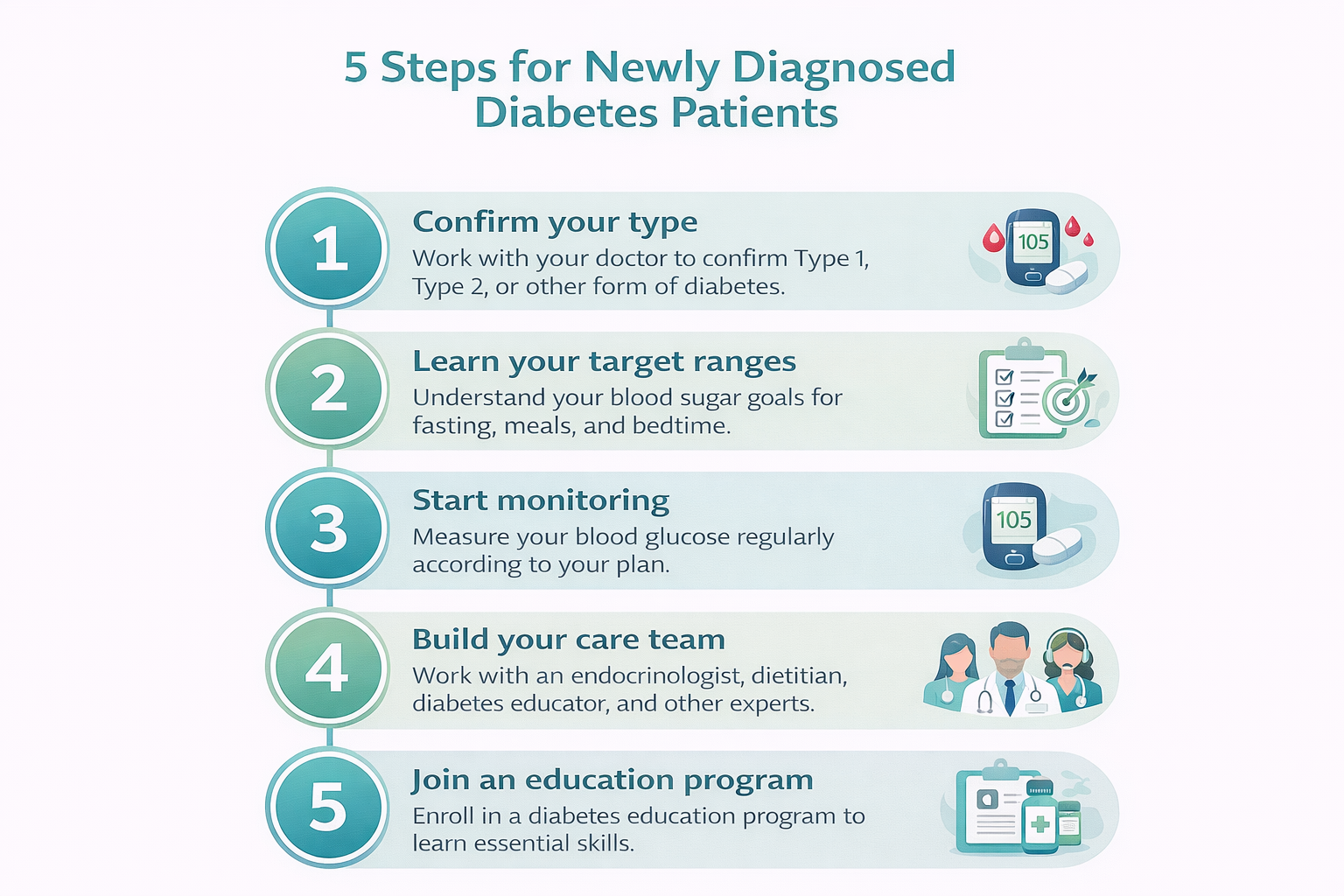
Your 5 First Steps After a Diabetes Diagnosis
- Confirm which type of diabetes you have. Type 1, Type 2, LADA, and other forms are managed differently — getting the right diagnosis matters.
- Learn your target blood sugar ranges. For most adults, the ADA recommends 80–130 mg/dL (4.4–7.2 mmol/L)
before meals and under 180 mg/dL (10.0 mmol/L) two hours after eating. - Start monitoring your blood sugar. Whether you use a traditional glucose meter or a continuous glucose monitor (CGM), regular testing shows how food, activity, and medication affect your glucose levels.
- Build your care team. Your primary care provider is a starting point, but you will benefit from a full team that includes a diabetes educator, dietitian, and possibly an endocrinologist.
- Ask about a diabetes education program. The ADA recommends Diabetes Self-Management Education and Support
(DSMES) for everyone newly diagnosed. Ask your doctor for a referral.
What Is Diabetes, and Why Does It Happen?
Diabetes is a condition in which your body has trouble managing blood sugar (glucose). Normally, a hormone called insulin — made by the pancreas — moves glucose from the bloodstream into your cells for energy. With diabetes, either the pancreas produces little or no insulin (Type 1), or the body does not use it effectively (Type 2), or a combination of both. The result is that blood sugar stays elevated, which over time can damage blood vessels and nerves throughout the body.
The good news is that keeping your blood sugar in a healthy range — through medication, diet, activity, and monitoring — dramatically reduces the risk of complications. Many people with diabetes lead full, active lives. Understanding how the condition works is the first step toward managing it confidently.
Understanding Your Risk and Diagnosis
Before or shortly after a diagnosis, many people wonder: Why did this happen to me? The answer depends on the type. Type 1 is an autoimmune condition with strong genetic components. Type 2 is influenced by lifestyle, age, family history, and ethnic background — but it is not simply a result of poor choices.
This article explains the key risk factors for each type of diabetes and describes the standard diagnostic tests your doctor uses — including the Fasting Plasma Glucose test, the Oral Glucose Tolerance Test, and the A1c test.
→ Read: Risk Factors and Diagnosis of Diabetes
What Type of Diabetes Do You Have?
Diabetes is not one condition — it is a family of conditions with different causes, progressions, and treatments. Type 1 and Type 2 are the most common, but LADA (sometimes called Type 1.5), gestational diabetes, MODY, and several rarer forms also exist. A misdiagnosis — particularly mistaking LADA for Type 2 — can delay the right treatment.
This article explains each major type in plain language, with a side-by-side comparison table and guidance on what tests to ask for if you are unsure your diagnosis is correct.
→ Read: Types of Diabetes Explained
How to Monitor Your Blood Sugar
Blood sugar monitoring is one of the most powerful tools you have. Testing gives you immediate feedback on how specific foods, activity levels, stress, and medication affect your glucose — information that lets you and your care team make smarter decisions.
This guide covers traditional fingerstick glucose meters and continuous glucose monitors (CGMs) — wearable sensors that track your glucose around the clock. It explains target ranges, when to test, and what to do when numbers are too high or too low.
→ Read: Blood Sugar Testing — A Guide for People with Diabetes
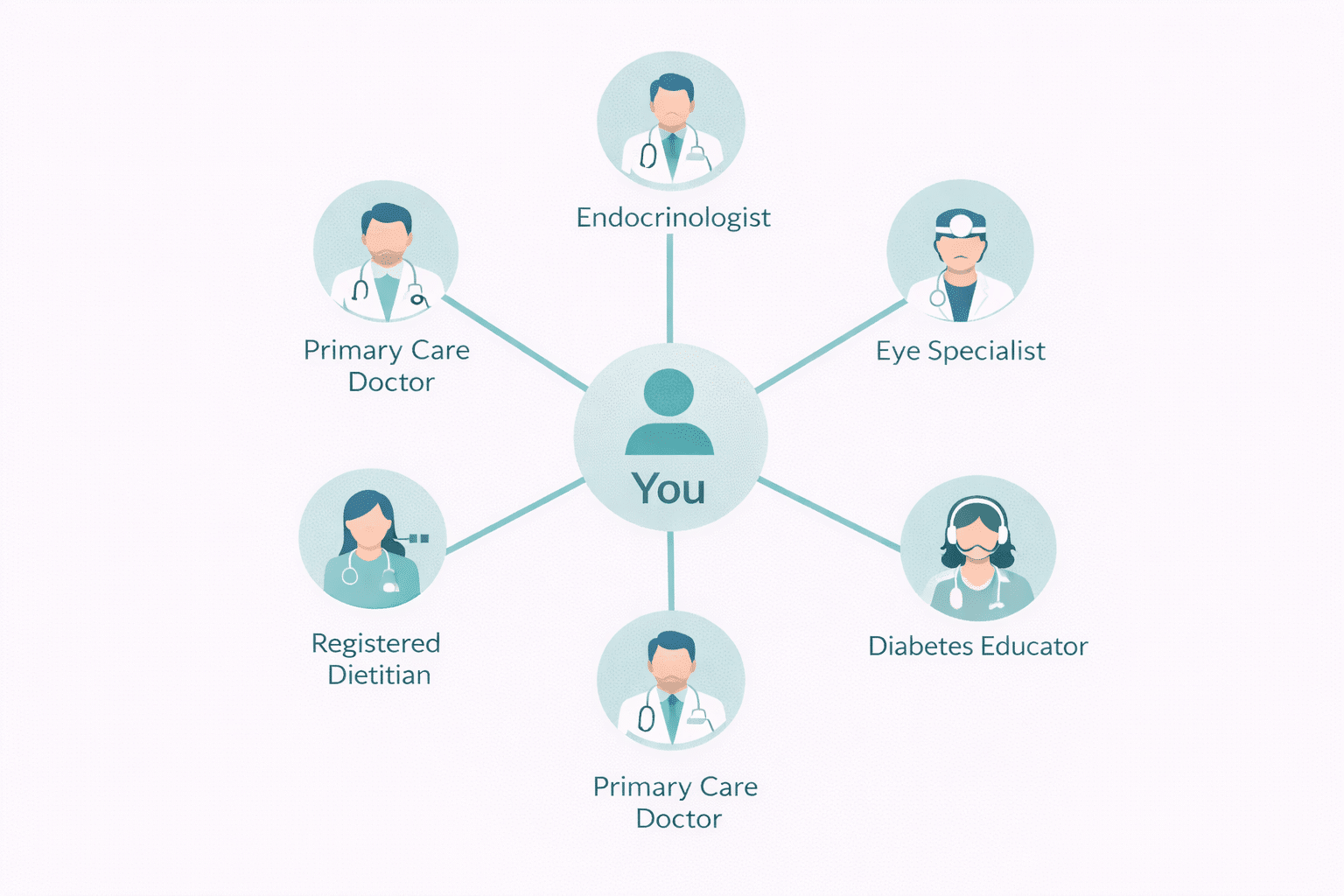
Your Diabetes Care Team and Healthcare Providers
Managing diabetes well is a team effort. This guide covers both what good diabetes care looks like — the routine appointments, tests, and check-ins you should expect — and who provides that care. You will learn the roles of your primary care provider, endocrinologist, certified diabetes care and education specialist (CDCES), registered dietitian, and other specialists.
It also includes practical guidance on communicating effectively with your doctors, including what questions to ask at your first appointment after diagnosis.
→ Read: Your Diabetes Care Team and Healthcare Providers
Eating Well After a Diabetes Diagnosis
Food affects your blood sugar more directly than almost anything else. But “eating for diabetes” does not mean a joyless or severely restricted diet. It means understanding how different foods — especially carbohydrates — raise your glucose, and making choices that keep your levels in range without sacrificing satisfaction.
This guide covers the most common evidence-based eating approaches for people with diabetes, including carb counting, the plate method, and low-glycemic eating. It is designed as an introduction — your registered dietitian will help you build a personalized plan.
→ Read: Diet and Nutrition After a Diabetes Diagnosis
Staying Motivated for the Long Term
Living with a chronic condition has emotional weight that is easy to underestimate at the start. Feelings of overwhelm, frustration, or burnout are common — and normal. The difference between people who thrive with diabetes and those who struggle often comes down not to knowledge or willpower, but to having the right strategies and support in place.
This guide covers practical, research-backed strategies for maintaining motivation over time, setting realistic goals, recognizing and addressing diabetes distress, and building the kind of day-to-day habits that make management feel sustainable rather than overwhelming.
→ Read: Staying Motivated with Diabetes
What Should I Expect in the First Year with Diabetes?
The first few months after a diagnosis are often the most intense. You are absorbing new information, adjusting routines, starting or changing medications, and learning what your body responds to. This is normal, and it does get easier. Here is a general picture of what to expect:
- First weeks: Focus on getting your blood sugar into a safer range. Your doctor may start or adjust medication right away. Learn to use your glucose meter or CGM and start tracking your readings.
- First 3 months: Your care team will check your A1c — a blood test that shows your average blood sugar over the past 2–3 months. The ADA recommends an A1c below 7% for most adults, though your personal target may differ.
- First year: You will have regular appointments to monitor how your treatment plan is working, check for early signs of complications, and adjust your approach as needed. Annual exams for your eyes, kidneys, and feet are standard.
- Ongoing: Diabetes management is not a one-time fix — it evolves as your life, health, and treatment options change. Staying informed and connected to your care team is the key to long-term success.
Helpful Resources and Research
The following organizations publish current guidelines and educational resources for people with diabetes:
- American Diabetes Association (ADA) Standards of Care 2026 — The clinical gold standard for diabetes diagnosis and management guidelines.
- Centers for Disease Control and Prevention — Diabetes Basics — Clear, accessible information on living with diabetes.
- American Association of Diabetes Care and Education Specialists (ADCES) — Find a certified diabetes educator near you.
- National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) — In-depth clinical information and research updates.
Frequently Asked Questions
These are the questions we hear most often from people who are newly diagnosed with diabetes.
What is the first thing I should do after a diabetes diagnosis?
Start by confirming which type of diabetes you have, since different types require different treatments. Then ask your doctor about a referral to a certified diabetes educator (CDCES) or a formal diabetes education program (DSMES). These programs are covered by most insurance and will give you a strong foundation for self-management. In the meantime, start tracking your blood sugar so you and your care team have data to work with.
What blood sugar level is considered diabetic?
A diabetes diagnosis is confirmed when a fasting blood sugar reaches 126 mg/dL (7.0 mmol/L) or higher, or when a random blood sugar is 200 mg/dL (11.1 mmol/L) or higher with symptoms, or when an A1c is 6.5% or above. Prediabetes is defined as a fasting blood sugar between 100–125 mg/dL (5.6–6.9 mmol/L) or an A1c of 5.7%–6.4%.
Will I have diabetes for the rest of my life?
For Type 1 diabetes, yes — it is a lifelong autoimmune condition that requires insulin. For Type 2 diabetes, some people are able to achieve remission (blood sugar returning to a non-diabetic range without medication) through significant weight loss and lifestyle changes, though the underlying susceptibility remains. Neither type disappears on its own, but both can be managed effectively to prevent complications and maintain quality of life.
Do I need to take medication right away?
It depends on your type and how high your blood sugar is. People with Type 1 diabetes require insulin from the start. For Type 2 diabetes, metformin is often prescribed at diagnosis alongside lifestyle changes, though your doctor may recommend starting with lifestyle changes alone if your blood sugar is only mildly elevated. Never stop or change prescribed medication without talking to your doctor first.
What is the difference between Type 1 and Type 2 diabetes?
Type 1 is an autoimmune disease where the body destroys the insulin-producing cells in the pancreas, resulting in little or no insulin production. It affects about 5–10% of people with diabetes and requires daily insulin. Type 2 is characterized by insulin resistance — the body makes insulin but cannot use it effectively — and accounts for 90–95% of cases. Type 2 is often managed with oral medications, lifestyle changes, and sometimes insulin.
How often should I check my blood sugar?
This depends on your type, treatment plan, and how stable your blood sugar is. People using insulin typically test more often — sometimes before every meal and at bedtime. People with Type 2 on oral medications alone may test less frequently. Your care team will give you a personalized testing schedule. If you use a continuous glucose monitor (CGM), it tracks your levels automatically every few minutes around the clock.
Can Type 2 diabetes be reversed?
Some people with Type 2 diabetes can achieve remission — meaning blood sugar returns to a normal range without medication — through significant lifestyle changes, particularly weight loss. This is most likely in people who have had Type 2 for a shorter time and who lose a substantial amount of weight (often 10–15% or more of body weight). Remission does not mean the condition has disappeared permanently, but it is a meaningful goal for many people.
What does the A1c test measure?
The A1c test (also called glycated hemoglobin or HbA1c) measures the percentage of red blood cells that have glucose attached to them. Because red blood cells live about 2–3 months, the A1c reflects your average blood sugar over that period. An A1c of 7% corresponds to an average blood sugar of roughly 154 mg/dL (8.6 mmol/L). Most adults with diabetes aim for an A1c below 7%, though your target may be higher or lower depending on your age, health status, and risk of low blood sugar.
Should I see an endocrinologist or is my primary care doctor enough?
Many people with Type 2 diabetes manage well with a primary care doctor, especially if their blood sugar is responding to treatment. However, an endocrinologist — a specialist in hormone conditions including diabetes — is recommended for people with Type 1 diabetes, those with Type 2 that is difficult to control, people on complex insulin regimens, or anyone experiencing frequent low or high blood sugar episodes. Your primary care provider can refer you.
What foods should I avoid after a diabetes diagnosis?
No single food is completely off-limits, but foods that raise blood sugar quickly and sharply are worth limiting. These include sugary drinks (regular soda, juice, energy drinks), refined carbohydrates (white bread, white rice, pastries), and foods high in both carbohydrates and saturated fat. A registered dietitian can help you build an eating plan that fits your preferences and keeps your blood sugar in range. Most people do best with an approach that is sustainable long-term rather than overly restrictive.
Last Updated on May 28, 2026