 The A1C test — also called the HbA1c test or average blood sugar test — is one of the most important lab tests in diabetes management, and understanding your result can make a real difference in your long-term health. Unlike your daily fingerstick readings that show what your blood sugar is at the moment, the A1C gives you the big picture: an estimate of your average blood sugar level over the past two to three months.
The A1C test — also called the HbA1c test or average blood sugar test — is one of the most important lab tests in diabetes management, and understanding your result can make a real difference in your long-term health. Unlike your daily fingerstick readings that show what your blood sugar is at the moment, the A1C gives you the big picture: an estimate of your average blood sugar level over the past two to three months.
A1C is a useful tool, but it’s only one part of glucose assessment — your daily readings and, if you use one, your continuous glucose monitor (CGM) data all work together to give a full picture. In this guide, you’ll learn what your A1C number means, what your personal target should be, what can influence the result, and the most practical ways to lower it.
Jump to: Frequently Asked Questions about the A1C Test ↓
A1C Levels at a Glance — What Does Your Number Mean?
Here’s a quick guide to help you understand your results. Your personal goal might be different from the general target — always talk with your care team to find the right number for you.
| A1C Level | Est. Average Blood Sugar | What It Means |
|---|---|---|
| Below 5.7% | Below 117 mg/dL (6.5 mmol/L) | Normal range |
| 5.7% – 6.4% | 117–137 mg/dL (6.5–7.6 mmol/L) | Prediabetes |
| 6.5% or higher | 140+ mg/dL (7.8+ mmol/L) | Diabetes diagnosis |
| Below 7% | Below 154 mg/dL (8.6 mmol/L) | ADA goal for most adults |
| 7% – 8% | 154–183 mg/dL (8.6–10.2 mmol/L) | May be appropriate for some (older adults, complex health) |
| Above your personal target | Varies | Discuss next steps with your care team — everyone’s personal target is different |
Source: ADA Standards of Care 2026, Section 6 — Glycemic Goals.
How Does the A1C Test Work?
Your red blood cells contain a protein called hemoglobin, which transports oxygen throughout your body. When blood sugar levels are high, glucose binds to hemoglobin — this process is known as glycation. The A1C test measures the percentage of your hemoglobin that has glucose attached to it.
Since red blood cells live for about 3 months, the test measures an average of your blood sugar over that entire period. Think of it like a weather report that shows the season’s average temperature instead of just today’s high. An A1C of 7% roughly equals an average blood sugar of about 154 mg/dL (8.6 mmol/L).
The test is performed with a simple blood draw — often right in your doctor’s office — and results are typically available within minutes or a few days, depending on the lab.
What Is a Good A1C Level for Someone with Diabetes?
The ADA’s 2026 Standards of Care recommend an A1C below 7% (53 mmol/mol) for most non-pregnant adults with diabetes. This target has been consistently associated with a significantly lower risk of complications, including eye disease, kidney damage, and nerve problems — findings first established by the landmark Diabetes Control and Complications Trial (DCCT) and the UK Prospective Diabetes Study (UKPDS).
That said, the right target for you is personal. Your care team may establish a different goal based on:
- Your age and overall health
- How long you’ve had diabetes
- Whether you use insulin or medications that can cause low blood sugar
- Your skill in recognizing and responding to low blood sugar
- Other health conditions you may have
Personalized A1C Goals
Here are the target ranges generally recommended by the ADA 2026 Standards of Care:
- Below 7% — suitable for most healthy, non-pregnant adults who are aware of low blood sugar
- Below 6.5% — suitable for most healthy adults and those newly diagnosed, especially those without a significant risk of low blood sugar (ADA 2026, Section 6)
- Below 8% — a reasonable goal for older adults with complex or multiple health conditions, a history of severe low blood sugar, or a shorter life expectancy
- Below 8% prior to elective surgery — new 2026 recommendation from ADA Section 16
The main point: a lower A1C isn’t always better for everyone. Pushing to achieve very low A1C levels can raise the risk of dangerous low blood sugar episodes. Your doctor should help you find a level that protects your long-term health without putting you at short-term risk. Those experiencing low glucose levels are eligible for a CGM, which allows accurate monitoring of the frequency and severity of these lows.
How Frequently Should You Check Your A1C?
According to ADA 2026 guidelines, how often you need an A1C test depends on how well your blood sugar is controlled:
- Twice a year — if your blood sugar is controlled and your treatment plan remains the same
- Every 3 months — if your blood sugar is not at goal, or if you have recently changed medications, insulin doses, or lifestyle habits
If you use a continuous glucose monitor (CGM), your device might calculate a ‘Glucose Management Indicator’ (GMI) — an ongoing estimate of your likely A1C level. This is a useful tool between lab visits, but it doesn’t replace an actual A1C blood test. A GMI is usually measured over the last 14 days and may not match the A1C that reflects the last three months, especially if your glucose levels have recently improved or worsened.
What Is Time in Range, and How Does It Relate to A1C?
If you use a CGM, your doctor might also discuss Time in Range (TIR) — the percentage of time your blood sugar stays between 70 and 180 mg/dL (3.9 to 10.0 mmol/L) throughout the day and night.
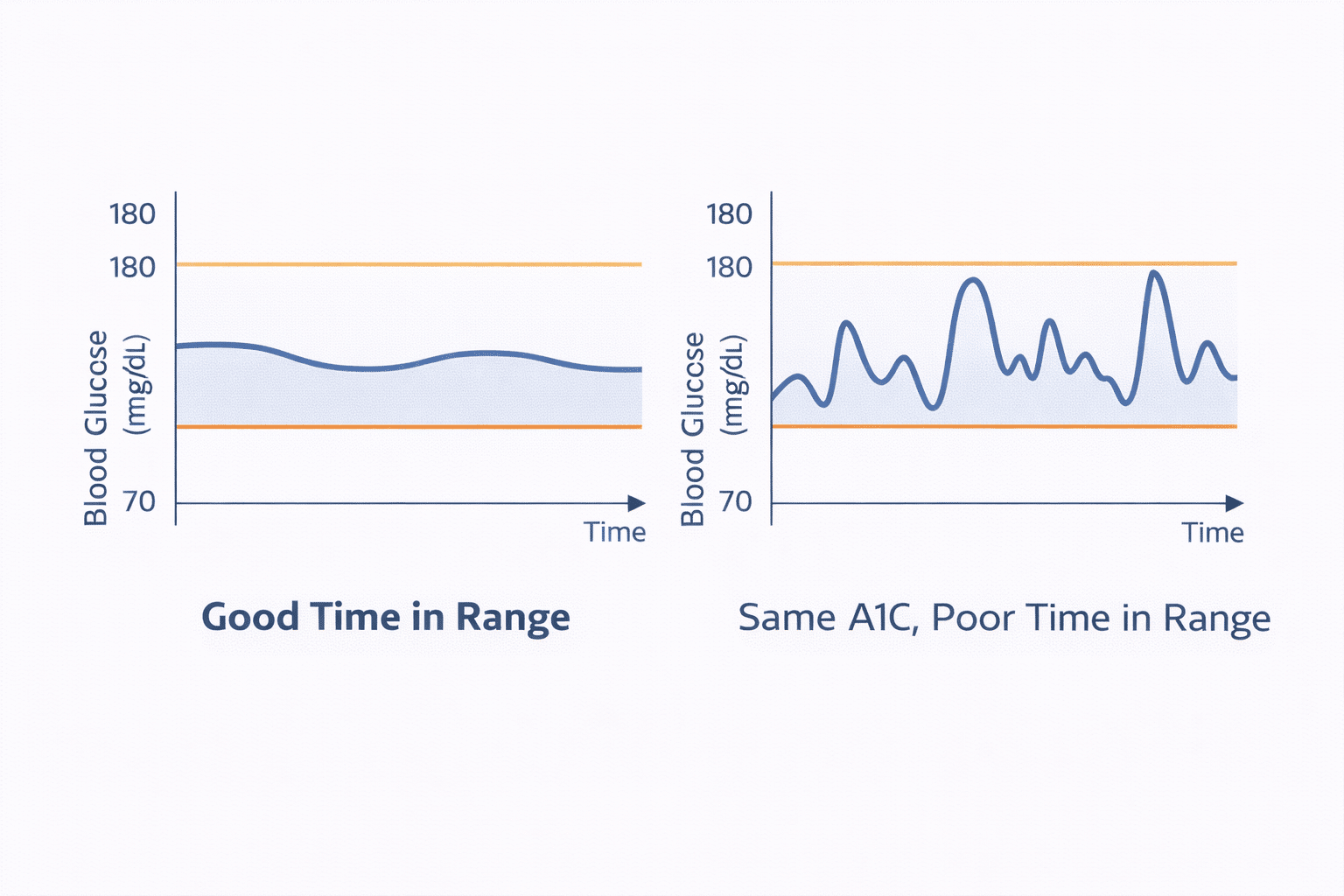
ADA 2026 guidelines now officially include TIR goals alongside A1C targets. Research indicates that spending more than 70% of the day in the range closely aligns with an A1C of around 7% (53 mmol/mol). This is important because A1C reflects the average blood sugar level, while TIR shows whether that average is steady or involves frequent highs and lows that cancel each other out.
For example, someone who spends equal time above 250 mg/dL (13.9 mmol/L) and below 70 mg/dL (3.9 mmol/L) could have an A1C of 7% that seems reassuring on paper — but their actual daily blood sugar fluctuations put them at real risk. CGM and TIR help reveal that picture.
| A1C Level | Time in Range Goal | Notes |
|---|---|---|
| ~ 7% (53 mmol/mol) | > 70% of the day | Most non-pregnant adults; ADA 2026 standard goal |
| ~ 8% (64 mmol/mol) | ≥ 50% of the day | Older adults with complex health or frailty |
Source: ADA Standards of Care 2026, Section 6; Battelino et al., Diabetes Care.
Note: TIR goals apply to CGM users. ADA 2026 recommends considering CGM from the time of diagnosis and later as needed, especially for people using insulin. If you don’t use a CGM yet, ask your care team if it might benefit you. Pregnancy has its own glycemic framework with distinct A1C and TIR targets — if you are pregnant or planning to become pregnant, discuss your personal goals with your care team separately.
What Factors Can Impact Your A1C Test Result?
The A1C test is reliable for most people, but certain medical conditions and situations can cause the result to seem higher or lower than your actual average blood sugar. Be sure to inform your doctor if any of the following apply to you:
- Iron deficiency anemia can falsely elevate your A1C.
- Sickle cell disease or other conditions affecting red blood cells can lead to inaccurate results in either direction.
- Chronic kidney disease can impact red blood cell lifespan and distort A1C results, often to abnormally low levels.
- Recent blood transfusions introduce new red blood cells that haven’t been exposed to your blood sugar, which can lower the measured A1C.
- Certain hemoglobin variants — more common in individuals of African, Mediterranean, or Southeast Asian descent — may interfere with some A1C testing methods.
- Liver disease and some medications, like certain HIV drugs and dapsone, can also impact A1C accuracy — always provide your care team with a complete picture of your health and medications.
If any of these apply to you, your care team might use additional tests — such as a fructosamine test or detailed CGM data — to monitor your blood sugar control instead.
How Can You Lower Your A1C Level?
If your A1C is above your personal goal, don’t be discouraged — there are practical, proven steps you can take. Even a modest reduction (such as dropping from 9% to 8%) significantly lowers your risk of complications. Here’s where to start:
1. Review Your Eating Habits
You don’t need to follow just one ‘diabetes diet,’ but your food choices directly affect your blood sugar. Here are a few strategies that consistently help:
- Distribute carbohydrates evenly throughout meals instead of consuming large amounts at once.
- Choose lower-glycemic carbohydrates like whole grains, legumes, and non-starchy vegetables instead of processed, high-sugar foods.
- Watch your portion sizes, especially for starchy foods like rice, bread, and potatoes.
- Limit sugar-sweetened drinks — even small amounts quickly raise blood sugar.
- Avoid already glycated proteins, such as honey-baked ham and beef jerky, which can raise A1C levels on their own.
 2. Get Moving More Often
2. Get Moving More Often

Physical activity helps your body use insulin more effectively, leading to better blood sugar control throughout the day. The ADA recommends at least 150 minutes of moderate activity each week, spread across most days, such as brisk walking, cycling, or swimming. Even short walks after meals can significantly reduce post-meal high blood sugar spikes.
One important note: if you take insulin or a sulfonylurea medication, exercise can increase your risk of low blood sugar during and after activity. Check your blood sugar before starting and consult your care team to see if you need to adjust your dose or have a snack nearby.
3. Take Medications Regularly
Whether you take oral medications, injectable medications like GLP-1 agonists, or insulin, maintaining consistency is extremely important. Missing doses — even occasionally — can cause blood sugar levels to rise, which then affects your A1C results over weeks and months. If cost, side effects, or scheduling issues make it hard to take your medications, talk to your doctor or pharmacist. There may be other options.
4. Monitor Your Blood Sugar Patterns
You can’t manage what you can’t see. Checking your blood sugar with a meter or using a continuous glucose monitor (CGM) helps you identify patterns — such as blood sugar rising after specific meals or dropping overnight — so you can make targeted adjustments instead of guessing. Many people find that seeing real-time data with a CGM motivates them to make changes that improve their A1C over time.
5. Manage Stress and Sleep
Stress hormones like cortisol can increase blood sugar levels, especially overnight and in the early morning. Long-term sleep deprivation also reduces insulin sensitivity. Although challenging, improving sleep quality and managing stress through activities such as walking, meditation, or maintaining consistent sleep hours can significantly improve your readings.
6. Keep Consistent with Follow-up Appointments
Regular check-ins with your care team help you catch rising trends early, before they worsen your A1C. If your A1C has been increasing between visits, addressing it at 7.5% is much easier than waiting until it reaches 9% or higher.

Does a Good A1C Indicate Your Blood Sugar Is Well-Controlled?
A low A1C is a positive sign, but it doesn’t tell the full story on its own. Since A1C is an average, it can look good even if your blood sugar swings between lows and highs often throughout the day.
That’s why contemporary diabetes management combines the A1C with three other tools:
- Daily blood sugar readings from a meter or CGM — showing individual highs and lows.
- Time in Range (TIR) from a CGM — showing how consistently your blood sugar stays in the healthy zone.
- Coefficient of variation (CV) from a CGM — showing your glucose variability (GV), the ups and downs in your readings. High variability makes it difficult to safely lower your glucose. Work with your clinician to keep your CV below 33%.
For example, a blood sugar reading before dinner of 145 mg/dL (8.0 mmol/L) followed by a 2-hour post-meal reading of 168 mg/dL (9.3 mmol/L) provides useful information that an A1C test cannot. Collectively, all four measures give you — and your doctor — the most complete picture of how your management is working.
Helpful Resources & Research
- ADA Standards of Care in Diabetes — 2026, Section 6: Glycemic Goals
- The DCCT Trial — foundational research on A1C and complication risk
- UKPDS — key study on type 2 diabetes and blood sugar control
- ADA eAG/A1C Conversion Calculator
- DiabetesNet.com — Continuous Glucose Monitors
- DiabetesNet.com — Low Blood Sugars
- DiabetesNet.com — High Blood Sugars
What does an A1C of 7% really indicate about my daily blood sugar levels?
An A1C of 7% reflects an estimated average blood sugar of about 154 mg/dL (8.6 mmol/L) over the past 2–3 months, based on data from the international ADAG study. Having an A1C around 7% has been linked to a lower risk of complications compared to higher A1C levels in major studies, such as the DCCT and UKPDS. Whether 7% is the right target for you depends on your individual situation — consult your doctor.
How soon can I expect my A1C to decrease?
Significant changes in A1C usually take about 3 months to appear in a test result, since it reflects roughly 3 months of blood sugar history. Many people notice meaningful improvements within that initial 3-month period, but the extent varies widely depending on your starting A1C, the treatment adjustments made, and how consistently those adjustments are followed. The most substantial improvements often occur in the first 3 to 6 months of a new treatment plan.
Is an A1C below 7% always the correct goal?
Not necessarily. While under 7% is the usual goal for most adults, the ADA 2026 guidelines emphasize that targets should be customized. Aiming for below 8% might be more appropriate for older adults, individuals with complex health issues, those on insulin who live alone, or those at high risk of severe low blood sugar episodes. Trying for a very low A1C can increase health risks for certain people.
Can the A1C test give a wrong result?
Yes, in some cases. Conditions that impact red blood cell lifespan — like anemia, sickle cell disease, chronic kidney disease, or recent blood transfusions — can cause the A1C to read higher or lower than your actual average blood sugar. If you have any of these conditions, talk with your doctor about alternative testing options, such as a fructosamine test or detailed CGM data.
How often should I get an A1C test?
The ADA recommends testing at least twice a year if your blood sugar is at goal and your treatment hasn’t changed. If your blood sugar isn’t well controlled or you’ve recently adjusted your medications, your doctor may want to test every 3 months to monitor your progress more closely.
What is Time in Range, and is it replacing the A1C?
Time in Range (TIR) does not replace the A1C — it complements it. TIR measures the percentage of time your blood sugar remains between 70 and 180 mg/dL (3.9–10.0 mmol/L), as tracked by a CGM device. ADA 2026 guidelines now officially recommend TIR goals alongside A1C. Aiming for more than 70% time in range generally corresponds to an A1C of about 7% (53 mmol/mol).
Can I lower my A1C through diet alone, without medication?
For some individuals — especially those newly diagnosed with type 2 diabetes and having modest A1C increases — significant improvements can be achieved through diet, exercise, and weight loss alone. Studies indicate that sustained weight loss of 10% or more can substantially reduce A1C and, in some cases, bring it close to normal levels. However, many people also require medication, and combining lifestyle modifications with appropriate treatment is generally the most effective strategy.
What’s the difference between A1C and eAG?
The Estimated Average Glucose (eAG) converts your A1C percentage into blood sugar units — the same mg/dL (or mmol/L) readings shown on your meter or CGM. For instance, an A1C of 7% corresponds to an eAG of roughly 154 mg/dL (8.6 mmol/L). Both the ADA and the American Association for Clinical Chemistry recommend that labs report both numbers together when an A1C is ordered, since many people find the blood sugar figure easier to understand.
Will using a CGM help lower my A1C?
Research consistently indicates that using a CGM is linked to lower A1C levels, especially for individuals on insulin. The real-time feedback from a CGM helps you identify blood sugar patterns that would otherwise go unnoticed between fingerstick tests. ADA 2026 recommends considering CGM from the time of diagnosis and later as needed, with a strong emphasis for those using insulin.
My A1C has increased since my last test. Does that mean I’ve failed?
Not at all. An A1C that’s trending upward provides information — it signals you and your care team that something in your management might need to change. Life events, stress, illness, changes in activity, or medication issues can all influence your A1C between tests. Instead of viewing a rise as a failure, see it as a sign to problem-solve with your doctor. Small, steady adjustments over time are how most people achieve lasting improvements.
Last Updated on April 14, 2026