Visit our BOB on a Pump page for more info about managing your BOB while on an insulin pump.
Bolus on Board (BOB) (also called Insulin on Board or Active Insulin) is the amount of rapid-acting insulin still working from recent boluses. Knowing your BOB is key to preventing bolus stacking and hypoglycemia—especially in the evening and at bedtime—because Humalog and Novolog can continue lowering glucose for 4 to 5 hours after a dose.
However, when boluses begin to overlap, a problem surfaces. How much insulin is still working from these recent injections or boluses? Humalog and Novolog continue to lower the blood sugar for four to five hours after they are given. Only by allowing for the long action time of rapid insulins can bolus stacking and hypoglycemia be avoided.
Determining BOB is especially important at bedtime. When several doses of rapid insulin are given during the evening hours, the bedtime blood sugar has to be interpreted in light of how much insulin is still left to work. A normal blood sugar at bedtime may be dangerous if a large residual insulin dose has yet to work. Likewise, a high reading at bedtime may require no additional bolus if sufficient BOB remains to take care of it.
Newer smart pumps have a Bolus On Board feature that can help solve this problem. Enter your blood sugar and the correction bolus you want to take. The pump will tell you how much unused or residual insulin you have left to act and will recommend an appropriate bolus that will not cause a low.
What Is Bolus on Board?
The Bolus on Board (also referred to as Insulin on Board or Active Insulin) tells how many units of rapid insulin are still working. This helps in deciding whether more insulin or more carbohydrate is needed. Never assume you need more insulin simply because your blood sugar is high at the moment. Always determine how much bolus is on board before taking more. If your blood sugar is normal with bolus on board, you may need to decide if carbohydrate is required to keep it normal.
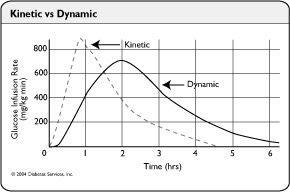
Rapid insulins are commonly perceived as faster than they really are. The kinetics of insulin are when that insulin can be measured in the bloodstream, whereas insulin’s dynamics are the time over which it will actually lower the blood sugar. After an injection, peak levels of Humalog and Novolog insulins are seen in the bloodstream about 45 minutes later, as shown by the dashed kinetic line to the right. The maximum effect on lowering the glucose level is not seen until 2 hours after injection or bolus and continues for over 4 to 5 hours. For more information on when these insulins really work, see our Kinetic vs Dynamic page.
From this, we get the Bolus on Board Rule for Humalog and Novolog:
20% of a dose will be used each hour after it is given
The table below provides an easy way to determine residual insulin. Be sure to discuss the use of this table with your physician.
| Insulin Left At 1, 2, 3, and 4 Hours After A Dose Of Humalog Or Novolog |
|||||||
|---|---|---|---|---|---|---|---|
| Dose Given | Units Left To Work After: | ||||||
| 1 Hr | 2 Hr | 3 Hr | 4 Hr | 5 Hr | |||
| 1 unit | 0.80 u | 0.60 u | 0.40 u | 0.20 u | 0 | ||
| 2 units | 1.60 u | 1.20 u | 0.80 u | 0.40 u | 0 | ||
| 3 units | 2.40 u | 1.80 u | 1.20 u | 0.60 u | 0 | ||
| 4 units | 3.20 u | 2.40 u | 1.60 u | 0.80 u | 0 | ||
| 5 units | 4.00 u | 3.00 u | 2.00 u | 1.00 u | 0 | ||
| 6 units | 4.80 u | 3.60 u | 2.40 u | 1.20 u | 0 | ||
| 7 units | 5.60 u | 4.20 u | 2.80 u | 1.40 u | 0 | ||
| 8 units | 6.40 u | 4.80 u | 3.20 u | 1.60 u | 0 | ||
| 9 units | 7.20 u | 5.40 u | 3.60 u | 1.80 u | 0 | ||
| 10 units | 8.00 u | 6.00 u | 4.00 u | 2.00 u | 0 | ||
Bolus On Board shows:
- how much insulin is still left to work from recent doses
- how much more insulin might be needed to lower a high blood sugar
- whether carbs may be needed to avoid a low because too much insulin is still left to work
Bolus On Board Tips:
- Be conservative when giving extra insulin, especially before bedtime. Take less insulin than usual if you are not going to be awake four hours later or set an alarm to test your blood sugar again at least 3 to 4 hours after the last bolus of the day was given.
- Try not to take a carb and correction boluses more often than every two hours unless there is a clear reason to do so. It takes at least two hours to get an indication of the effect of the last bolus.
- Always determine how much bolus is on board when you test two hours after you eat. What appears to be a high reading may resolve itself before the next meal once the residual insulin has acted.
- If Bolus on Board, your post-meal correction scale or other means give different estimates for how much insulin you should take, use the one that recommends the smaller bolus.
Bolus on Board is accurate only if you use a basal and bolus approach to your insulin doses, and your TDD, basals, and your carb and correction factors have been accurately set.
Examples:
Example One: Let’s say Joe’s blood sugar is above the maximum number on his meter, somewhere above 450 mg/dl (25 mmol), after he forgot to cover several slices of pizza with Humalog. Luckily no ketones are present.
Joe’s blood sugar drops 40 points per unit (his TDD is 45 units), so he takes 9 units of Humalog to bring down the high reading. Two hours later, he rechecks his blood sugar and now finds it measures 344 mg/dl (19.1 mmol). Does he need to take another dose of Humalog?
Using the table above, he finds that of the 9 units he took, 9 units X .60% or 5.4 units of Humalog are left to work. Since his blood sugar drops 40 points (2.2 mmol) on each unit of Humalog, he can estimate how many more points the remaining 5.4 units of residual insulin will lower his blood sugar:
5.4 units left times 40 points per unit = 216 mg/dl (12 mmol) left to drop
So Joe knows his blood sugar is likely to drop another 216 points. Since his blood sugar is 344 (19.1 mmol), he can expect to be at 344 – 216, or 128 mg/dl (7.1 mmol) in about 3 more hours when the last of the 9 unit injection is used up.
Joe knows he will need additional Humalog to finish correcting his high blood sugar. To reach his target of 100 from 200 and drop the remaining 28 mg/dl, he will need:
28 points ÷ 40 points per unit = 0.7 more units
Joe can now make an informed decision:
- During the day, he might take .7 units (visually estimating).
- Near bedtime or during the night, he might take only half a unit to get closer to his target without causing a nighttime low.
Example Two: Loren goes out for breakfast at a new restaurant. After ordering pancakes and fruit, she delays taking her Humalog until the food arrives so she can more accurately estimate the carbohydrate content. When her plate arrives, she estimates 100 grams of carbohydrate and takes 9 units of Humalog (her TDD is 45 units, and she uses 1 H for every 11 grams of carbohydrate).
However, two hours later, she finds that her blood glucose measures 272 mg/dL (11.1 mmol/L). Her blood glucose decreases by 40 points per unit of Humalog. Does she need to do anything about this high blood sugar?
To find out, let’s see how much of the 9 units taken for breakfast is still working using the table. After 2 hours, about 40% of the nine units are gone (20 percent times 2 hours), leaving 40% of the meal dose left to work. The table shows 9 units times 0.6 equals 5.4 units still remaining to work.
So 5.4 units times a drop of 40 mg/dl per unit tells Loren she is likely to drop an additional 216 points. When her breakfast injection is totally gone, her blood sugar should be 272 minus 216 points or 56 mg/dl.
This suggests Loren’s high blood sugar will come down without additional insulin. A follow-up blood sugar in 60 minutes will clarify whether this is happening. Loren may actually need a small amount of carbohydrate to avoid a low blood sugar before lunch.
This last example shows clearly why you need to think when using insulin. It takes at least two hours to get an idea of what the last carb or high blood sugar injection is doing if you are using Humalog. Taking extra insulin too soon after a meal can create an excess accumulation of insulin, complicate your unused insulin calculations, and create situations where insulin reactions become likely.
The example also illustrates a problem that may arise when eating out. In this situation, Loren’s post-meal blood sugar rises higher than a desirable target of 140 or 150 mg/dl (7.8 to 8.3 mmol) at two hours. Her carbohydrate-rich breakfast raised her blood sugar even though she may have taken a slightly excessive dose of Humalog. This is partly because of the quick-acting pancakes and partly because the dose was taken just before beginning to eat.
In many situations, like going out for a pancake breakfast, it helps to lead the meal with a partial injection taken a half-hour early. Keep glucose tablets available as needed.
Pumping Insulin provides extensive information and is the most helpful book ever written on insulin use.
Using Insulin takes you step by step toward excellent control. Whether you use one injection and pills, or six injections, you’ll learn far more from this book than from any other!
Last Updated on December 31, 2025