 Metabolic syndrome and diabetes are closely linked conditions, with insulin resistance — your body’s cells not responding properly to insulin — a major underlying driver of both. Also known as Syndrome X or Insulin Resistance Syndrome, metabolic syndrome is a cluster of five risk factors that together significantly raise your chances of developing type 2 diabetes, heart disease, and stroke.
Metabolic syndrome and diabetes are closely linked conditions, with insulin resistance — your body’s cells not responding properly to insulin — a major underlying driver of both. Also known as Syndrome X or Insulin Resistance Syndrome, metabolic syndrome is a cluster of five risk factors that together significantly raise your chances of developing type 2 diabetes, heart disease, and stroke.
You don’t need to have all five risk factors to be at risk. If you have just three, you meet the clinical definition of metabolic syndrome. According to the American Heart Association, about one-third of U.S. adults have metabolic syndrome. Many don’t realize it. The good news is that lifestyle changes and, when necessary, medication can greatly reduce your risk of developing type 2 diabetes.
Jump to: Frequently Asked Questions about Metabolic Syndrome
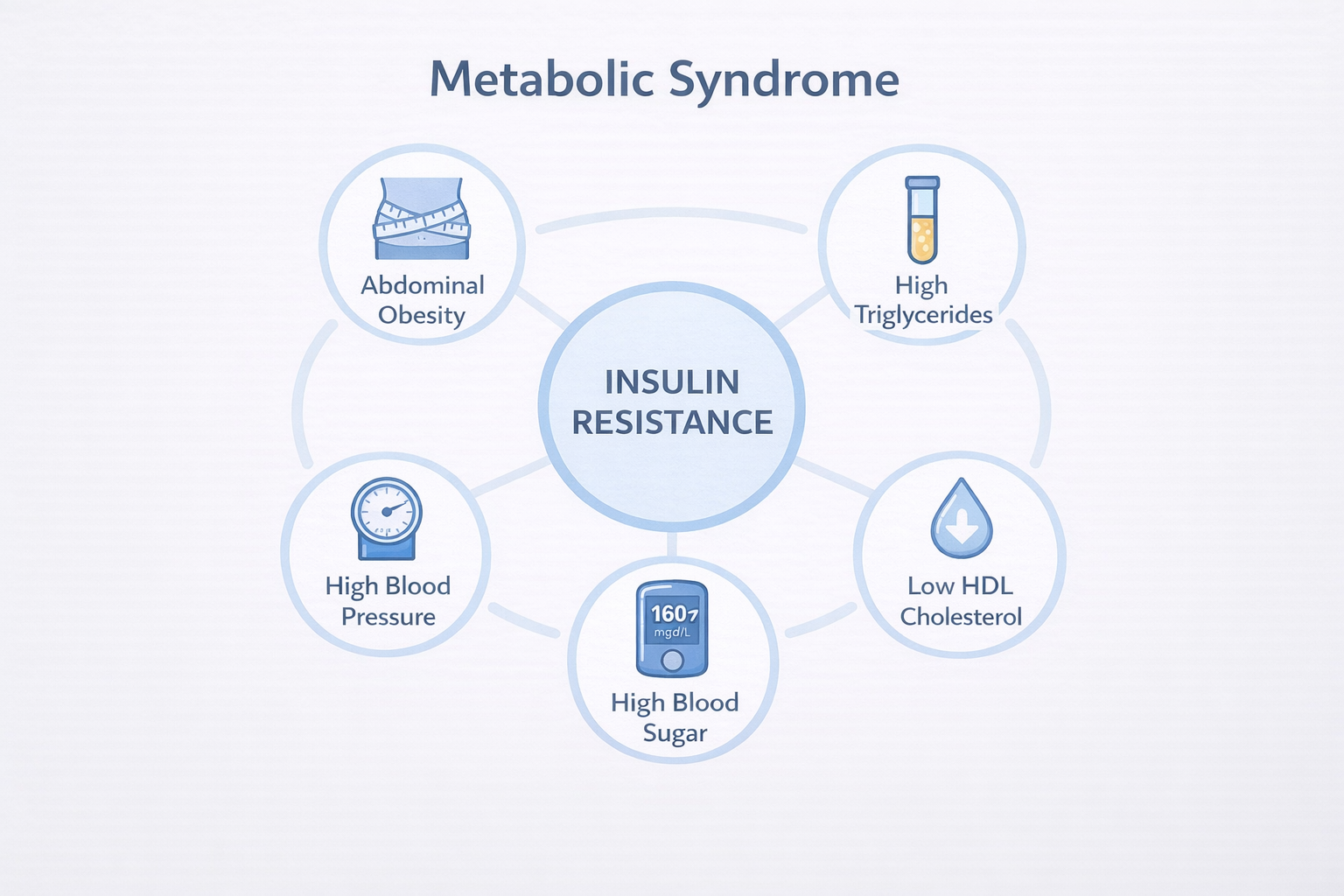
The 5 Signs of Metabolic Syndrome
Metabolic syndrome is diagnosed when you have three or more of the following:
| Risk Factor | Threshold (Men) | Threshold (Women) |
|---|---|---|
| Waist circumference (abdominal obesity) | > 40 inches (102 cm) | > 35 inches (88 cm) |
| High triglycerides | ≥ 150 mg/dL (1.7 mmol/L) | ≥ 150 mg/dL (1.7 mmol/L) |
| Low HDL (“good”) cholesterol | < 40 mg/dL (1.0 mmol/L) | < 50 mg/dL (1.3 mmol/L) |
| High blood pressure | ≥ 130/85 mmHg | ≥ 130/85 mmHg |
| High fasting blood sugar | ≥ 100 mg/dL (5.6 mmol/L) | ≥ 100 mg/dL (5.6 mmol/L) |
Commonly used U.S. criteria reflected by AHA/NHLBI guidance.
What Is Syndrome X and Why Does It Have So Many Names?
Syndrome X, metabolic syndrome, and Insulin Resistance Syndrome are closely related terms that are often used interchangeably in patient education, although they are not exactly the same concepts. It is also important to note that “Syndrome X” has a different meaning in cardiology, where it refers to chest pain with normal coronary arteries (also called cardiac syndrome X or microvascular angina) — a completely different condition. Dr. Gerald Reaven first described the metabolic cluster and its connection to insulin resistance and cardiovascular risk in a landmark 1988 lecture at Stanford University (not in the 1960s or 1990s, as some older articles claim), and the condition has had several names since then. Today, most doctors and guidelines refer to it as “metabolic syndrome,” which is the term used throughout this article.
The “syndrome” part simply means it’s a group of conditions that tend to occur together — not a single disease. Insulin resistance is the common factor: when your cells stop responding well to insulin, your body compensates by producing more insulin, which triggers a chain reaction that affects your blood sugar, blood pressure, cholesterol, and body weight.
How Does Metabolic Syndrome Increase Your Risk of Diabetes?
Insulin resistance is central to both metabolic syndrome and type 2 diabetes. Here’s how the progression usually unfolds:
- Your muscle, fat, and liver cells no longer respond effectively to insulin.
- Your pancreas compensates by producing more insulin to maintain your blood sugar levels.
- Over time, your insulin-producing cells become overworked and begin to lose their function.
- Blood sugar levels start to rise, first into the prediabetes range (100–125 mg/dL / 5.6–6.9 mmol/L), then into the type 2 diabetes range (≥ 126 mg/dL / 7.0 mmol/L on two fasting tests).
People with metabolic syndrome are estimated to be about fivefold more likely to develop type 2 diabetes than those without it, according to many studies, including a systematic review and meta-analysis by Mottillo et al. (Circulation, 2010). The risk increases even further when combined with a family history of diabetes or a sedentary lifestyle. Detecting metabolic syndrome early provides a crucial opportunity to slow or prevent this progression.
Already managing blood sugar? People with prediabetes or type 2 diabetes who also have metabolic syndrome face an increased cardiovascular risk. This is why the current ADA Standards of Care 2026 (Section 10) recommend addressing all components of metabolic syndrome, not just blood sugar, in people with diabetes.
What Are the Symptoms of Metabolic Syndrome?
Most components of metabolic syndrome produce no obvious symptoms, which is why it often goes undiagnosed. The exception is abdominal obesity, which is visible and measurable. Here’s what to know about each component:
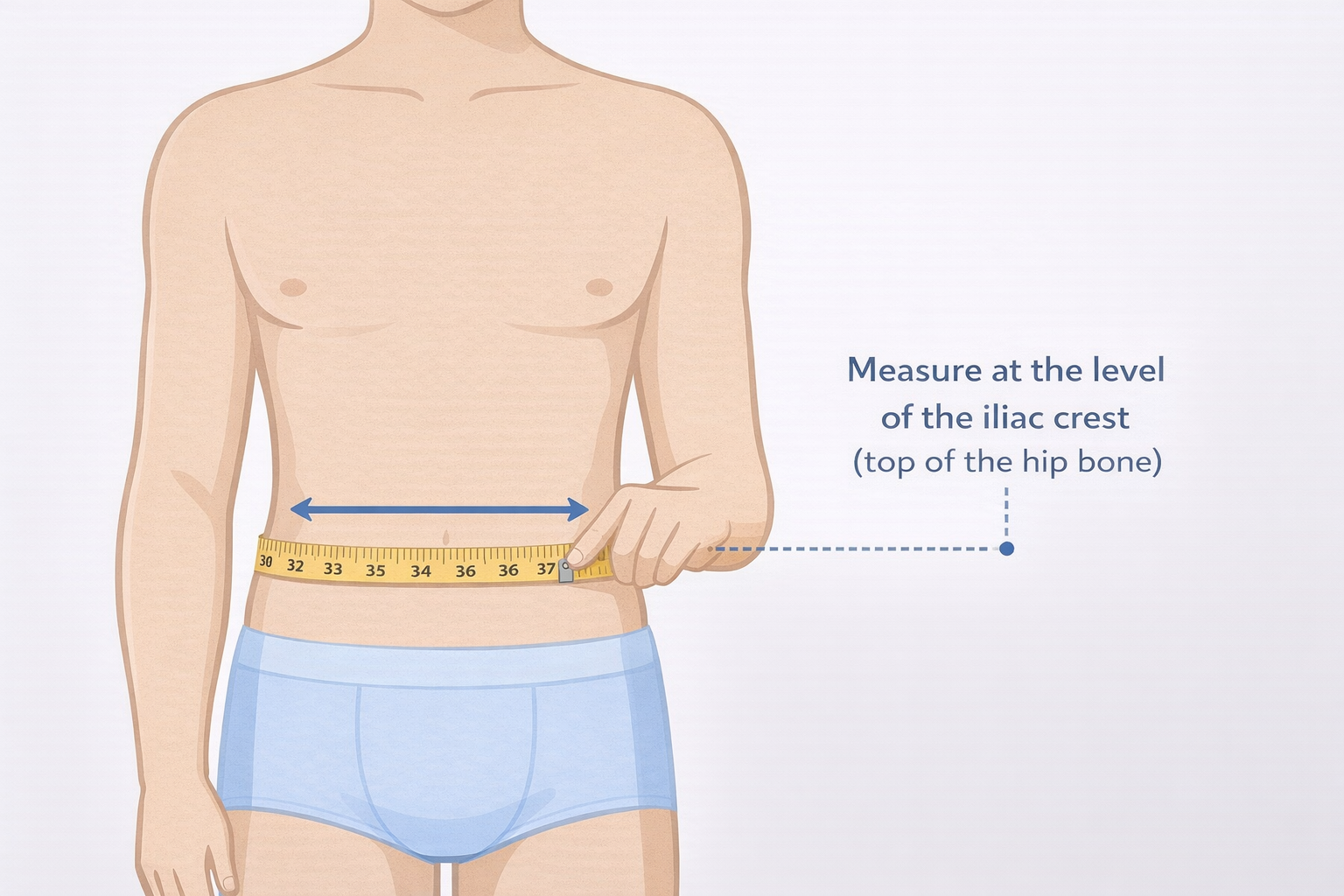
Abdominal Obesity
Excess fat around the waist — sometimes called an “apple shape” — is one of the strongest predictors of insulin resistance. This internal fat around organs (visceral fat) is metabolically active and releases hormones that cause inflammation and interfere with how your cells respond to insulin. Waist circumference is measured at the level of the iliac crest (the top of your hip bone), which is the standard method used by the NHLBI.
High Triglycerides
Triglycerides are the primary type of fat in your blood. Levels of 150 mg/dL (1.7 mmol/L) or higher indicate a warning. Elevated triglycerides often increase alongside insulin resistance because excess insulin promotes fat storage.
Low HDL Cholesterol
HDL (“good”) cholesterol helps clear other types of cholesterol from your blood. Low HDL levels are linked to a higher risk of heart disease. In metabolic syndrome, low HDL often occurs with high triglycerides — a combination sometimes called “dyslipidemia.”
High Blood Pressure
Blood pressure of 130/85 mmHg or higher is the threshold under current criteria. Insulin resistance contributes to high blood pressure by causing the kidneys to retain more sodium and by promoting the constriction of blood vessels.
High Fasting Blood Sugar
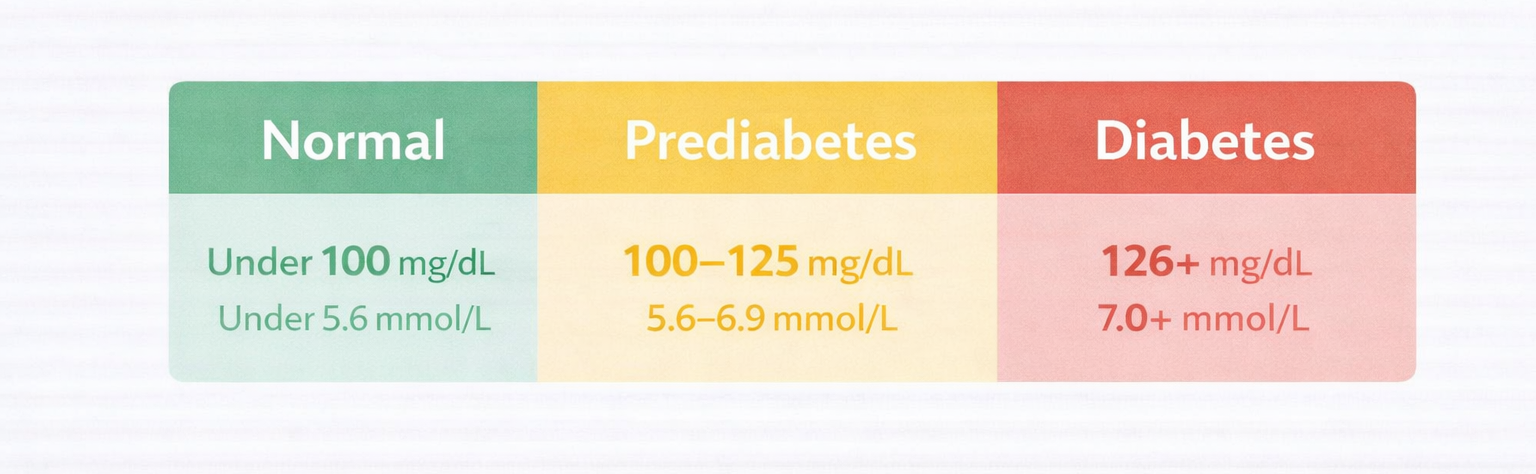
A fasting blood sugar level of 100 mg/dL (5.6 mmol/L) or higher, but not yet in the diabetes range, is considered prediabetes. This is the clearest warning that insulin resistance is impacting your blood sugar control. If your fasting blood sugar reaches 126 mg/dL (7.0 mmol/L) or higher on two separate tests, that indicates you have type 2 diabetes.
Who Is Most at Risk for Metabolic Syndrome?
Metabolic syndrome affects about one-third of U.S. adults, with recent NHANES analyses indicating that prevalence may be increasing. The risk rises with age, but it’s not confined to older adults. Several groups face a higher-than-average risk:
| Risk Factor | Why It Matters |
|---|---|
| Age 50+ | Prevalence increases sharply after age 50; over 40% of adults 60+ are affected |
| Hispanic/Latino heritage | Higher rates of abdominal obesity and insulin resistance compared to other groups |
| South Asian heritage | Higher visceral fat at lower BMI values; standard waist thresholds may underestimate risk |
| Family history of diabetes | Genetic predisposition to insulin resistance increases overall syndrome risk |
| Polycystic ovary syndrome (PCOS) | Strongly associated with insulin resistance, women with PCOS have an elevated risk of metabolic syndrome |
| Physical inactivity | A sedentary lifestyle is a major modifiable driver of insulin resistance |
| Smoking | Contributes to insulin resistance and inflammation; compounds cardiovascular risk |
How Is Metabolic Syndrome Diagnosed?
There is no single blood test for metabolic syndrome. Your doctor diagnoses it by checking for three or more of the five risk factors listed in the quick reference table above. Routine lab work that includes a fasting glucose and lipid panel (for triglycerides), along with a blood pressure reading and waist measurement, provides your doctor with everything needed to make the diagnosis.
The Role of the Glucose Tolerance Test
A fasting blood glucose test is the most common screening method. If your fasting blood sugar is borderline, your doctor may recommend a glucose tolerance test (GTT), which involves drinking a measured sugar solution and having your blood taken at scheduled intervals. This test can identify impaired glucose tolerance earlier than fasting glucose alone in some individuals. A fasting blood sugar between 100–125 mg/dL (5.6–6.9 mmol/L) indicates prediabetes; 126 mg/dL (7.0 mmol/L) or higher suggests type 2 diabetes.
Early on, most people who are insulin-resistant still produce enough insulin to keep their fasting blood sugar within the normal range. The GTT can detect this earlier by measuring how the body handles a sugar load over two hours.
Continuous Glucose Monitoring as an Emerging Tool
Some clinicians may use continuous glucose monitoring (CGM) off-label to better understand post-meal blood sugar patterns in people with insulin resistance who have normal fasting values. Current ADA guidance recommends CGM mainly for people already managing diabetes, so this is not yet a standard diagnostic method for metabolic syndrome. It can provide a more complete view of how your blood sugar behaves throughout the day, but whether it is appropriate for you is a conversation to have with your doctor.
Can Metabolic Syndrome Be Reversed?
Yes — in many cases, metabolic syndrome can be significantly improved or even reversed through lifestyle changes, especially if detected early. The ADA Standards of Care 2026 (Section 5) stress that intensive lifestyle intervention is the key treatment for insulin resistance and metabolic syndrome.
A landmark study, the Diabetes Prevention Program (DPP), found that people with prediabetes and insulin resistance who lost 5–7% of their body weight and exercised 150 minutes per week reduced their risk of developing type 2 diabetes by 58% — outperforming metformin, which reduced the risk by 31%.
Lifestyle Changes That Have the Biggest Impact
- Weight loss: Even a 5–10% reduction in body weight can significantly improve all five components of metabolic syndrome.
- Physical activity: Aim for at least 150 minutes of moderate activity each week, such as brisk walking. Resistance training also enhances insulin sensitivity.
- Dietary changes: Cutting back on refined carbs and added sugars, boosting fiber intake, and adopting a Mediterranean-style eating pattern are all backed by strong evidence.
- Quit smoking: Smoking increases insulin resistance and significantly raises cardiovascular risk when combined with metabolic syndrome.
- Alcohol reduction: Cutting back on heavy drinking lowers triglycerides and blood pressure, promoting overall metabolic health.
How Is Metabolic Syndrome Managed with Medication?
When lifestyle changes alone are insufficient, your doctor might prescribe medication to target individual aspects of metabolic syndrome. Treatment generally focuses on the specific risk factors that are elevated. Note that there is no single medication approved for metabolic syndrome as a whole condition — each component is addressed separately.
| Component | Common Medication Options | Notes |
|---|---|---|
| High blood sugar / prediabetes | Metformin | Used selectively in high-risk prediabetes patients per ADA guidance; not universally recommended for metabolic syndrome as a condition |
| High blood sugar (type 2 diabetes) | GLP-1 agonists, SGLT-2 inhibitors | Both drug classes also reduce cardiovascular and kidney risk. GLP-1 and other incretins assist in weight loss. |
| High triglycerides | Fibrates, omega-3 fatty acids | Often improves with weight loss and reducing sugar intake first |
| High blood pressure | ACE inhibitors, ARBs, thiazide diuretics | ACE inhibitors and ARBs may have added kidney-protective benefits in diabetes |
| Low HDL cholesterol | Exercise and dietary changes are most effective; raising HDL with niacin did not improve cardiovascular outcomes in major trials and is not recommended | Focus on statins and other medications that reduce overall ASCVD risk |
In people with obesity and/or type 2 diabetes, GLP-1 receptor agonists such as semaglutide and tirzepatide have demonstrated improvements in several cardiometabolic risk factors associated with metabolic syndrome, including body weight, waist circumference, blood pressure, and triglycerides. Although they are not approved specifically for metabolic syndrome as an official indication, their wide-ranging effects on multiple components make them an increasingly valuable option for individuals who have both type 2 diabetes and features of metabolic syndrome. Clinical trial data supporting these effects have been published in the New England Journal of Medicine, among other journals.
Helpful Resources & Research
- ADA Standards of Medical Care in Diabetes — 2026
- American Heart Association: Metabolic Syndrome
- National Heart, Lung, and Blood Institute: Metabolic Syndrome
- Diabetes Prevention Program Outcomes Study (DPPOS)
- Reaven GM. Role of Insulin Resistance in Human Disease. Diabetes. 1988;37(12):1595–1607. doi: 10.2337/diab.37.12.1595.
- Grundy SM, Cleeman JI, Daniels SR, Donato KA, Eckel RH, Franklin BA, Gordon DJ, Krauss RM, Savage PJ, Smith SC Jr, Spertus JA, Costa F. Diagnosis and Management of the Metabolic Syndrome: An American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Circulation. 2005;112(17):2735–2752. doi: 10.1161/CIRCULATIONAHA.105.169404.
- Mottillo S, Filion KB, Genest J, et al. The Metabolic Syndrome and Cardiovascular Risk: A Systematic Review and Meta-Analysis. J Am Coll Cardiol. 2010;56(14):1113-1132. doi:10<.1016/j.jacc.2010.05.034
What is metabolic syndrome, and is it the same as Syndrome X?
These terms are often used interchangeably in patient education to describe a cluster of five risk factors: abdominal obesity, high triglycerides, low HDL cholesterol, high blood pressure, and high blood sugar. Insulin resistance is a key driver linking them. Note that “Syndrome X” also has a separate meaning in cardiology (chest pain with normal coronary arteries), so “metabolic syndrome” is the preferred and clearer modern term.
How many risk factors do I need to be diagnosed with metabolic syndrome?
You need at least three of the five criteria — abdominal obesity, high triglycerides, low HDL cholesterol, high blood pressure, or high fasting blood sugar — to meet the clinical definition of metabolic syndrome. Even one or two risk factors should prompt a conversation with your doctor about your cardiovascular and diabetes risk.
Does metabolic syndrome mean I will get type 2 diabetes?
Not automatically, but metabolic syndrome significantly raises your risk. Research, including a major meta-analysis (Mottillo et al., Circulation 2010), estimates the risk is about fivefold higher than in people without it. The Diabetes Prevention Program showed that modest weight loss and regular exercise can cut the risk of progressing from prediabetes to type 2 diabetes by 58%.
Can metabolic syndrome be reversed?
Yes, in many cases. Losing 5–10% of your body weight and getting 150 minutes of moderate exercise per week can reverse individual components or eliminate the diagnosis entirely. The ADA Standards of Care 2026 (Section 5) identify intensive lifestyle intervention as the first-line treatment for insulin resistance and metabolic syndrome.
What fasting blood sugar level indicates metabolic syndrome?
A fasting blood sugar of 100 mg/dL (5.6 mmol/L) or higher is one of the five metabolic syndrome criteria. Levels between 100–125 mg/dL (5.6–6.9 mmol/L) indicate prediabetes; 126 mg/dL (7.0 mmol/L) or above on two separate tests indicates type 2 diabetes. Always consult your doctor for a proper diagnosis.
Is metabolic syndrome more common in certain ethnic groups?
Yes. Hispanic/Latino Americans and South Asian Americans have higher rates of metabolic syndrome, even at lower body weights. South Asians in particular tend to develop insulin resistance and abdominal obesity at lower BMI thresholds than standard guidelines suggest, which is why some clinicians use adjusted waist circumference cutoffs for this population.
What does insulin resistance mean?
Insulin resistance means your cells don’t respond as well as they should to insulin, the hormone that moves sugar from your blood into your cells for energy. Think of insulin as a key, and your cells as locked doors — insulin resistance means the key no longer opens the door easily. Over time, the extra demand on your pancreas can cause blood sugar levels to rise, eventually leading to prediabetes or type 2 diabetes.
Can you have metabolic syndrome without being overweight?
Yes. You can have metabolic syndrome at a normal body weight, especially if you carry excess visceral fat (fat around the organs) without visible obesity. This is particularly common in people of South Asian descent, who tend to develop insulin resistance at lower BMI levels. Some clinicians use adjusted waist circumference thresholds for higher-risk populations.
What medications are used to treat metabolic syndrome?
There is no single drug approved specifically for metabolic syndrome. Doctors treat each component separately: metformin (selectively, for high-risk prediabetes), GLP-1 agonists or SGLT-2 inhibitors (for type 2 diabetes), fibrates or omega-3s (for high triglycerides), and ACE inhibitors or ARBs (for high blood pressure). GLP-1 receptor agonists are increasingly valuable because they address weight, blood pressure, and triglycerides alongside blood sugar.
Should I be screened for metabolic syndrome even if I feel fine?
Yes. Most components of metabolic syndrome cause no symptoms until significant damage has already occurred. A routine checkup that includes a fasting blood glucose test, a lipid panel, a blood pressure reading, and a waist measurement gives your doctor everything needed to assess your risk. The ADA and AHA both recommend periodic screening for anyone with one or more risk factors.
Last Updated on April 7, 2026