Men and diabetes is a topic that doesn’t get enough attention. While diabetes affects men and women roughly equally, men often face a distinct set of symptoms and complications — and are less likely to seek help until problems become serious. Understanding how diabetes affects men specifically, and what the latest research says, is the first step toward better management and fewer long-term complications.
Jump to: Frequently Asked Questions
📋 Quick Summary: Diabetes in Men
- Unique symptoms: Men with diabetes are more than 3 times more likely to experience erectile dysfunction (ED) than men without diabetes. ED may also be an early warning sign of cardiovascular disease.
- Hormonal health: Low testosterone is common in men with Type 2 diabetes and can worsen insulin resistance. It is worth discussing with your doctor.
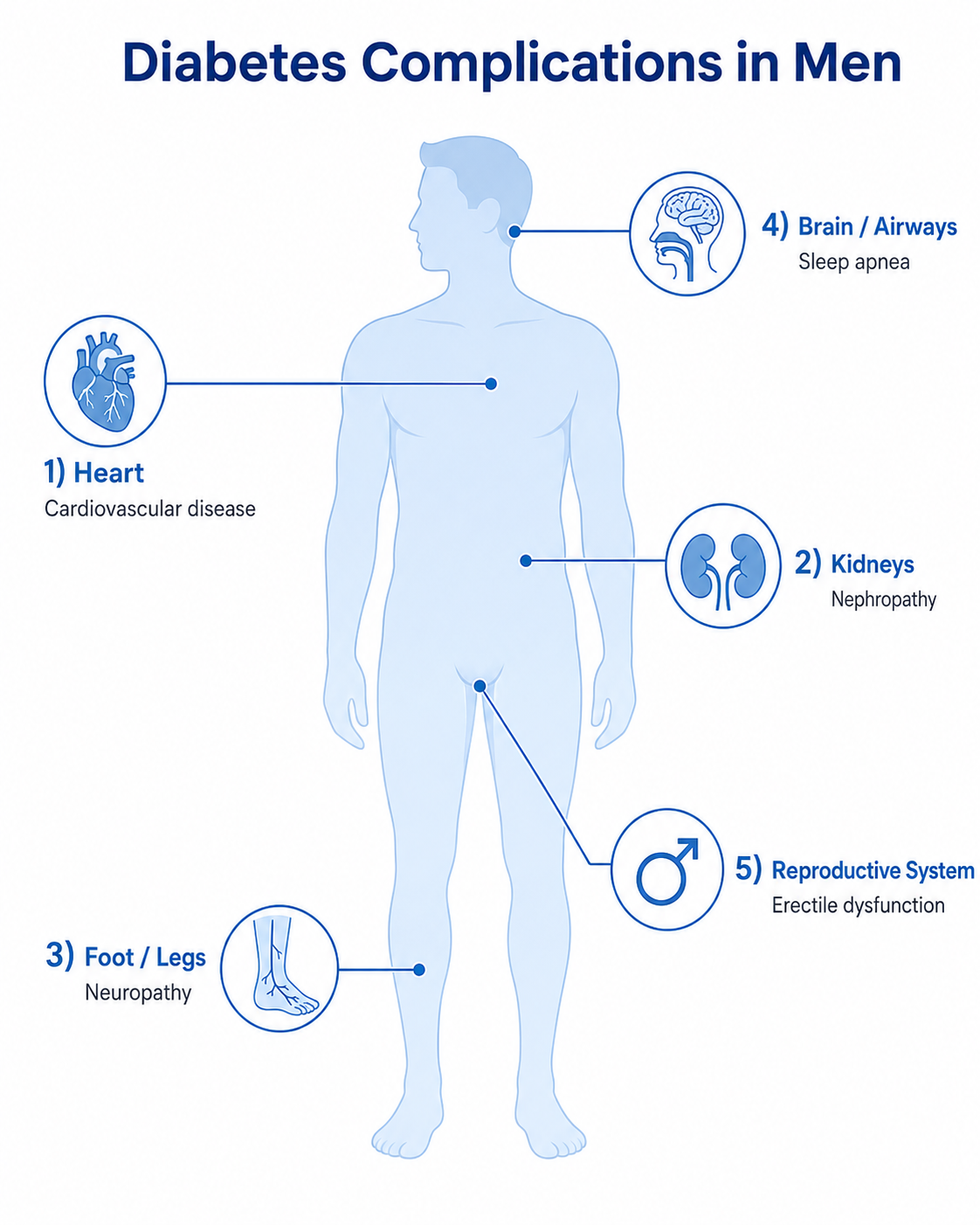
- Complication risk: Men may develop certain complications — particularly cardiovascular disease, kidney disease, and foot problems — earlier, or be diagnosed later than women.
- Mental health: Men with diabetes have higher rates of depression and diabetes distress — and are less likely to report symptoms or seek help.
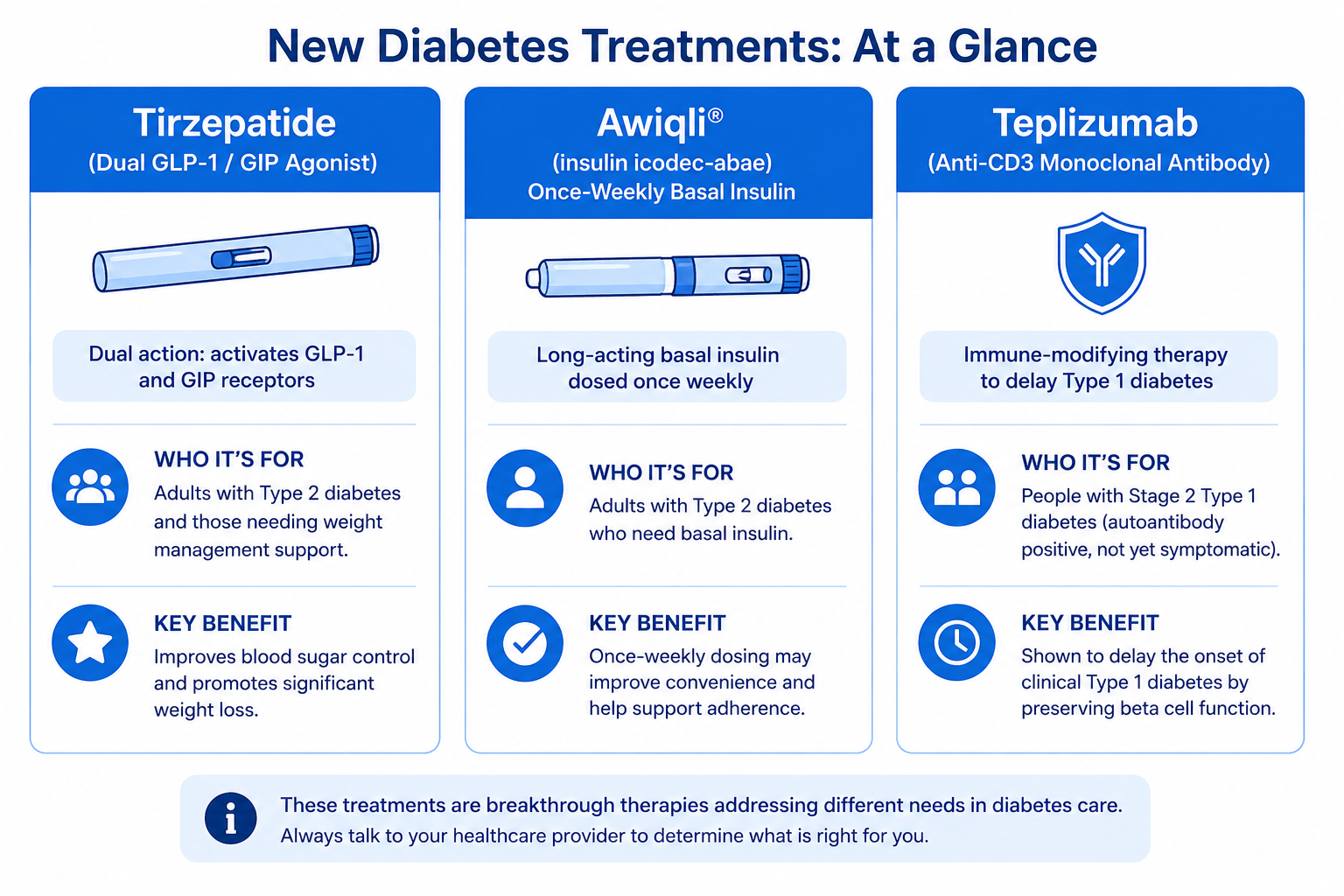
- Latest treatments: Tirzepatide, insulin icodec-abae (Awiqli), and teplizumab represent significant recent advances in diabetes care.
What are the symptoms of diabetes in men?
The classic symptoms of diabetes appear in both men and women: frequent urination, increased thirst, unexplained weight loss, fatigue, and blurred vision. But men also experience several complications that are specific to male biology — and these are often the first sign that something is wrong.
Erectile dysfunction (ED)
Erectile dysfunction is one of the most common — and most underreported — complications of diabetes in men. Research published in 2025 estimates that the prevalence of ED is more than 3.5 times higher in men with diabetes compared to men without the condition. Among men with long-standing diabetes, ED may affect up to 75%.
The mechanism involves both nerve damage and reduced blood flow. Diabetes damages the small blood vessels and nerves that control erections, making it harder to achieve or maintain one.
ED as a cardiovascular signal: Research has consistently shown that men with diabetes who develop ED have a significantly higher risk of heart attack and stroke. ED shares the same underlying pathology as coronary artery disease — damaged blood vessels — and often appears years before a cardiac event. If you have diabetes and are experiencing ED, bring it up with your doctor as a cardiovascular concern, not just a personal one.
Low testosterone (hypogonadism)
Men with Type 2 diabetes have significantly higher rates of low testosterone than the general male population. Low testosterone contributes to:
- Reduced muscle mass and strength
- Increased body fat, particularly around the abdomen
- Fatigue and low energy
- Decreased sex drive
- Mood changes, irritability, or depression
The relationship between testosterone and diabetes runs in both directions: low testosterone worsens insulin resistance, and high blood sugar reduces testosterone production.
Important: Testosterone therapy is generally considered only when low morning testosterone is confirmed on repeat testing and symptoms are present. It is not a diabetes treatment by itself, and current evidence does not show that it reliably improves blood sugar control. Discuss testing and any treatment options with your doctor before proceeding.
Retrograde ejaculation
High blood sugar over time can damage the nerves that control ejaculation. In some men, this leads to retrograde ejaculation, where semen enters the bladder instead of exiting during orgasm. While not dangerous, it can affect fertility. If you and your partner are trying to conceive, discuss this with a urologist.
Urinary and genital infections
Elevated blood sugar creates conditions that support the growth of yeast and bacteria. Men with diabetes — particularly uncircumcised men — have a higher risk of balanitis (inflammation of the foreskin and glans), fungal infections, and urinary tract infections. Keeping blood sugar in range significantly reduces this risk.
What complications are men with diabetes most at risk for?
| Complication | What Men Should Know |
|---|---|
| Heart disease & stroke | Men with diabetes develop heart disease earlier than women, partly because they lack the protective effect of estrogen. High blood sugar damages arteries, and the risk compounds with high blood pressure, high cholesterol, and smoking. ED is often the first warning sign. |
| Kidney disease | Studies show men are at higher risk of kidney disease progression compared to women with diabetes. Regular kidney function screening (urine albumin and eGFR) is essential. |
| Nerve damage (neuropathy) | Diabetic neuropathy commonly presents as numbness, tingling, burning pain, or loss of protective sensation in the feet and legs. Untreated, it increases amputation risk. Men also tend to seek foot care later than women. |
| Sleep apnea | Obstructive sleep apnea is significantly more common in men and is directly linked to insulin resistance. Treating sleep apnea may improve blood sugar control and cardiovascular health. |
| Depression & mental health | Men with diabetes have higher rates of depression, anxiety, and diabetes distress. They are also less likely to seek help. Mental health directly affects glucose control — and deserves the same attention as physical complications. |
What are the latest diabetes treatments for men?
Research continues to advance rapidly. Here are the most significant recent developments relevant to men managing diabetes:
Tirzepatide (Mounjaro / Zepbound)
GLP-1 receptor agonists like tirzepatide (Mounjaro for Type 2 diabetes, Zepbound for weight management) work on two hormone pathways simultaneously — GLP-1 and GIP. Clinical trials show tirzepatide reduces A1c by 1.5–2.5% on average and supports significant weight loss, which can improve insulin sensitivity, testosterone levels, and cardiovascular risk factors in men.
Insulin icodec-abae (Awiqli) — once-weekly basal insulin
In March 2026, the FDA approved insulin icodec-abae (brand name Awiqli) as the first once-weekly basal insulin for adults with Type 2 diabetes. For men who find daily injections difficult to maintain, a once-weekly option may reduce the management burden. One important caution: because each dose covers seven days, dosing errors or missed doses have more prolonged effects than with daily basal insulin. Careful education and follow-up with your care team are essential when starting Awiqli.
Teplizumab (Tzield) for Type 1 diabetes
Teplizumab is the first FDA-approved drug to delay the onset of Type 1 diabetes in people who are at high risk but haven’t yet progressed to it. FDA labeling now includes adults and children age 1 year and older with Stage 2 Type 1 diabetes — meaning they test positive for diabetes-related autoantibodies and have abnormal glucose levels, but have not yet developed full clinical symptoms. It is given as a 14-day intravenous infusion and can delay progression to clinical Type 1 by two years or more in eligible individuals.
Automated insulin delivery (AID) systems
The ADA 2026 Standards of Care designate AID systems as the preferred insulin delivery method for people with Type 1 diabetes and for adults with Type 2 diabetes on intensive insulin therapy. These systems combine a CGM with an insulin pump that automatically adjusts delivery based on real-time glucose readings, reducing both high and low blood sugar episodes.
What are the most effective management strategies for men with diabetes?
- Strength training + aerobic exercise: Both improve insulin sensitivity, but strength training has an additional benefit for men — it supports testosterone levels and helps maintain muscle mass. Aim for at least 150 minutes of moderate aerobic activity per week, plus 2 resistance training sessions. See the exercising with diabetes guide for practical advice.
- Monitor testosterone and hormonal health: If you’re experiencing fatigue, low sex drive, weight gain, or mood changes, ask for a morning testosterone test. If confirmed low on repeat testing, discuss causes and options with your doctor — lifestyle changes such as weight loss, exercise, and improved sleep often improve levels meaningfully.
- Prioritize sleep: Poor sleep and sleep apnea both raise cortisol and blood sugar. If you snore or wake up unrefreshed, ask your doctor about a sleep study.
- Address mental health directly: Diabetes distress — feeling overwhelmed or burned out by managing diabetes — is as common as clinical depression in people with diabetes. A diabetes care and education specialist (DCES) or a mental health professional who understands chronic illness can help significantly.
- Watch for nutritional gaps: Men with diabetes commonly have low vitamin D, B12, and magnesium — all of which can affect energy, nerve function, and blood sugar. Ask your doctor about testing.
- Don’t skip preventive care: Annual foot exams, eye exams, kidney function tests, and cardiovascular screening are not optional with diabetes — early detection of complications is far easier to treat than advanced ones. Men are statistically less likely to attend routine appointments, and that gap has real consequences.
⚠️ Medical disclaimer: This article is for educational purposes and does not replace medical care. For urgent symptoms such as chest pain, severe low blood sugar, confusion, or signs of stroke, seek emergency care immediately. Medications including testosterone therapy and weekly insulin require individualized medical supervision.
Helpful Resources & Research
- ADA Standards of Care in Diabetes — 2026
- Erectile Dysfunction in Diabetes Mellitus: A Narrative Review (Wiley, 2025)
- CDC: Men and Diabetes
- American Diabetes Association: Men’s Health
- NIDDK: Sexual and Urologic Problems in Men with Diabetes
- FDA: Novel Drug Approvals 2026 (Awiqli)
Frequently Asked Questions — Men and Diabetes
Is erectile dysfunction a sign of diabetes?
It can be. Men with diabetes are more than 3.5 times as likely to develop ED as men without diabetes. Because ED and cardiovascular disease share the same underlying cause — damaged blood vessels — ED in a man with diabetes may signal an elevated risk of heart disease. Bring it up with your doctor as a health concern, not just a personal one.
Does diabetes cause low testosterone?
There is a strong association between Type 2 diabetes and low testosterone. Insulin resistance and low testosterone worsen each other. If you have fatigue, reduced muscle mass, low sex drive, or mood changes, ask your doctor to check your testosterone levels with a morning blood test. Testosterone therapy is appropriate only when low levels are confirmed and symptoms are present — it is not a diabetes treatment by itself.
Why are men with diabetes at higher cardiovascular risk?
Men generally develop cardiovascular disease earlier than women, partly because estrogen offers women some protection in younger years. Diabetes increases this risk by damaging blood vessels, raising blood pressure and cholesterol, and promoting inflammation. Men with diabetes who also have ED face particularly elevated cardiovascular risk because both conditions share the same root cause.
What is the best exercise for men with diabetes?
A combination of aerobic exercise and strength training is most effective. Aerobic exercise (brisk walking, cycling, and swimming) improves insulin sensitivity within hours. Strength training builds muscle — the body’s primary glucose-disposal organ — and supports testosterone levels over time. Aim for at least 150 minutes of moderate activity per week, with resistance training at least twice weekly.
Can I take ED medications if I have diabetes?
PDE5 inhibitors (sildenafil/Viagra, tadalafil/Cialis, vardenafil/Levitra) are commonly used and generally safe for men with diabetes who do not have serious cardiovascular disease or take nitrate medications. Talk to your doctor before starting any ED medication to ensure it is appropriate for your cardiovascular profile. Improving blood sugar control addresses the underlying cause.
What is Awiqli and how is it different from daily insulin?
Awiqli (insulin icodec-abae) is the first once-weekly basal insulin, approved by the FDA in March 2026 for adults with Type 2 diabetes. Each injection covers seven days, reducing the daily injection burden. The trade-off is that dosing errors or missed doses have longer-lasting effects than with daily insulin, so careful education and close monitoring at the start are important.
Does sleep apnea really affect blood sugar?
Yes. Obstructive sleep apnea — significantly more common in men — causes repeated drops in blood oxygen during sleep, raising cortisol and adrenaline, both of which increase blood sugar and reduce insulin sensitivity. Treating sleep apnea with CPAP therapy has been shown to improve blood sugar control, blood pressure, and overall cardiovascular health in people with diabetes.
What mental health resources are available for men with diabetes?
Diabetes distress — feeling overwhelmed or burned out from managing diabetes — is extremely common and distinct from clinical depression, though both require attention. A diabetes care and education specialist (DCES) can help with the practical burden, while a therapist who specializes in chronic illness can address the emotional side. Ask your care team for a referral.
Can I father children if I have diabetes?
Most men with diabetes can father children. The main concerns are erectile dysfunction (treatable), retrograde ejaculation (manageable with specialist help), and reduced sperm quality linked to oxidative stress from high blood sugar. Keeping blood sugar well controlled improves fertility. If you’re having difficulty conceiving, a urologist or fertility specialist can evaluate the specific factors involved.
What is teplizumab and who is it for?
Teplizumab (Tzield) is the first FDA-approved drug to delay the onset of Type 1 diabetes. It is now approved for adults and children aged 1 year and older with Stage 2 Type 1 diabetes — meaning they test positive for diabetes-related autoantibodies and have abnormal glucose, but have not yet developed clinical symptoms. It is given as a 14-day intravenous infusion and can delay progression by two or more years in eligible individuals.
Last Updated on June 2, 2026