Understanding diabetes risk factors and how a diagnosis is made is one of the most important first steps after receiving a diabetes diagnosis — or after being told you may be at risk. This guide explains what increases the likelihood of developing Type 1 or Type 2 diabetes, walks through each standard diagnostic test and what your results mean, and covers prediabetes — a common and often overlooked warning sign that offers real options for prevention.
The short answer: Doctors diagnose diabetes using an A1c test, a fasting plasma glucose test, an oral glucose tolerance test, or — when symptoms are obvious — a random glucose test. All adults should begin screening for prediabetes and Type 2 diabetes at age 35, or earlier if you are overweight or obese, plus at least one other risk factor. If results are normal, re-testing at least every 3 years is recommended.
Read on for what each test involves, what your numbers mean, and what to do next.
Jump to: Frequently Asked Questions ↓
What Are the Blood Sugar Thresholds for Prediabetes and for Diabetes?
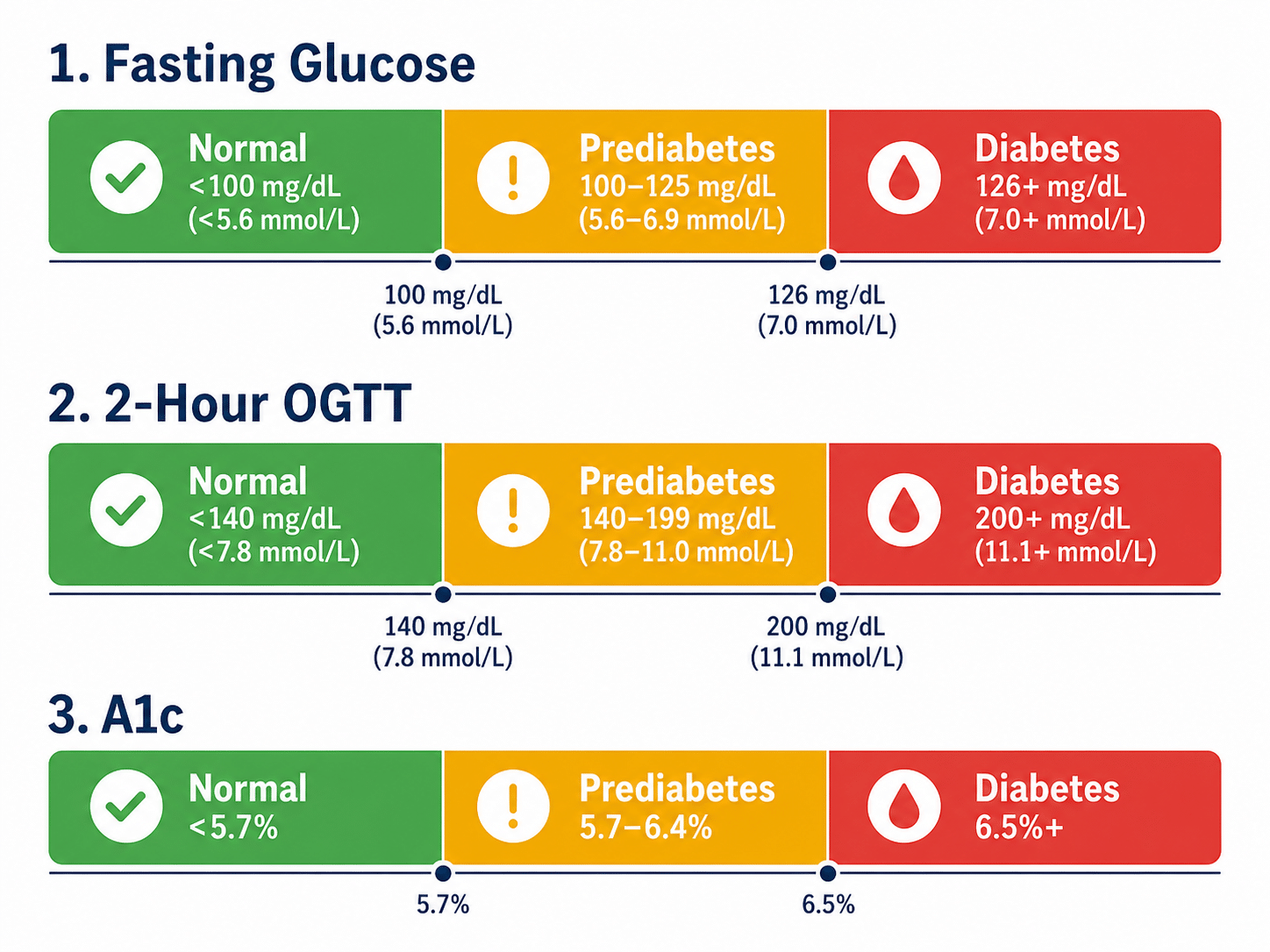
Here is a quick-reference summary of the thresholds your doctor uses to interpret each test. All values are based on the ADA Standards of Care 2026.
| Test | Normal | Prediabetes | Diabetes |
|---|---|---|---|
| Fasting Plasma Glucose (FPG) | Below 100 mg/dL (5.6 mmol/L) | 100–125 mg/dL (5.6–6.9 mmol/L) | 126 mg/dL (7.0 mmol/L) or higher |
| 2-Hour OGTT | Below 140 mg/dL (7.8 mmol/L) | 140–199 mg/dL (7.8–11.0 mmol/L) | 200 mg/dL (11.1 mmol/L) or higher |
| A1c (HbA1c) | Below 5.7% | 5.7%–6.4% | 6.5% or higher |
| Random Glucose with Symptoms | N/A | N/A | 200 mg/dL (11.1 mmol/L) or higher |
One result is usually not enough: The ADA recommends confirming an abnormal result with a repeat test on a different day, unless you have clear symptoms and a random glucose of 200 mg/dL (11.1 mmol/L) or higher, or two different tests taken at the same time both meet the diagnostic threshold. A single borderline result should always be discussed with your doctor before conclusions are drawn.
What Are the Risk Factors for Type 1 Diabetes?
Type 1 diabetes is an autoimmune disease in which the immune system attacks and destroys the insulin-producing beta cells in the pancreas. It is not caused by diet, lifestyle, or body weight. Researchers believe Type 1 develops in genetically susceptible individuals after environmental triggers, but no single trigger has been proven to cause most cases. The mechanisms involved remain an active area of research.
Genetic factors
Genetics plays a meaningful but incomplete role in Type 1 risk. The strongest genetic associations involve the HLA-DR and HLA-DQ regions of DNA. However, genetics alone does not determine outcome. Most people newly diagnosed with Type 1 diabetes do not have a first-degree relative with the condition, suggesting that environmental factors — not genetics alone — play a significant role in triggering the disease.
Who should consider screening for Type 1 risk?
The ADA 2026 Standards now recommend offering autoantibody-based screening for presymptomatic Type 1 diabetes to individuals with a family history of Type 1 diabetes or a known high genetic risk. TrialNet provides free risk screening for first-degree relatives of people with Type 1 diabetes ages 2–45, and for second-degree relatives ages 2–20. If you or a family member may be eligible, visit TrialNet.org for details.
What Are the Risk Factors for Type 2 Diabetes?
 Type 2 diabetes develops when the body becomes insulin-resistant, and the pancreas can no longer compensate. Unlike Type 1, Type 2 is strongly associated with lifestyle, metabolic, and genetic factors. The ADA 2026 Standards of Care recommend that all adults begin screening at age 35, with earlier screening for those who are overweight or obese and have one or more additional risk factors.
Type 2 diabetes develops when the body becomes insulin-resistant, and the pancreas can no longer compensate. Unlike Type 1, Type 2 is strongly associated with lifestyle, metabolic, and genetic factors. The ADA 2026 Standards of Care recommend that all adults begin screening at age 35, with earlier screening for those who are overweight or obese and have one or more additional risk factors.
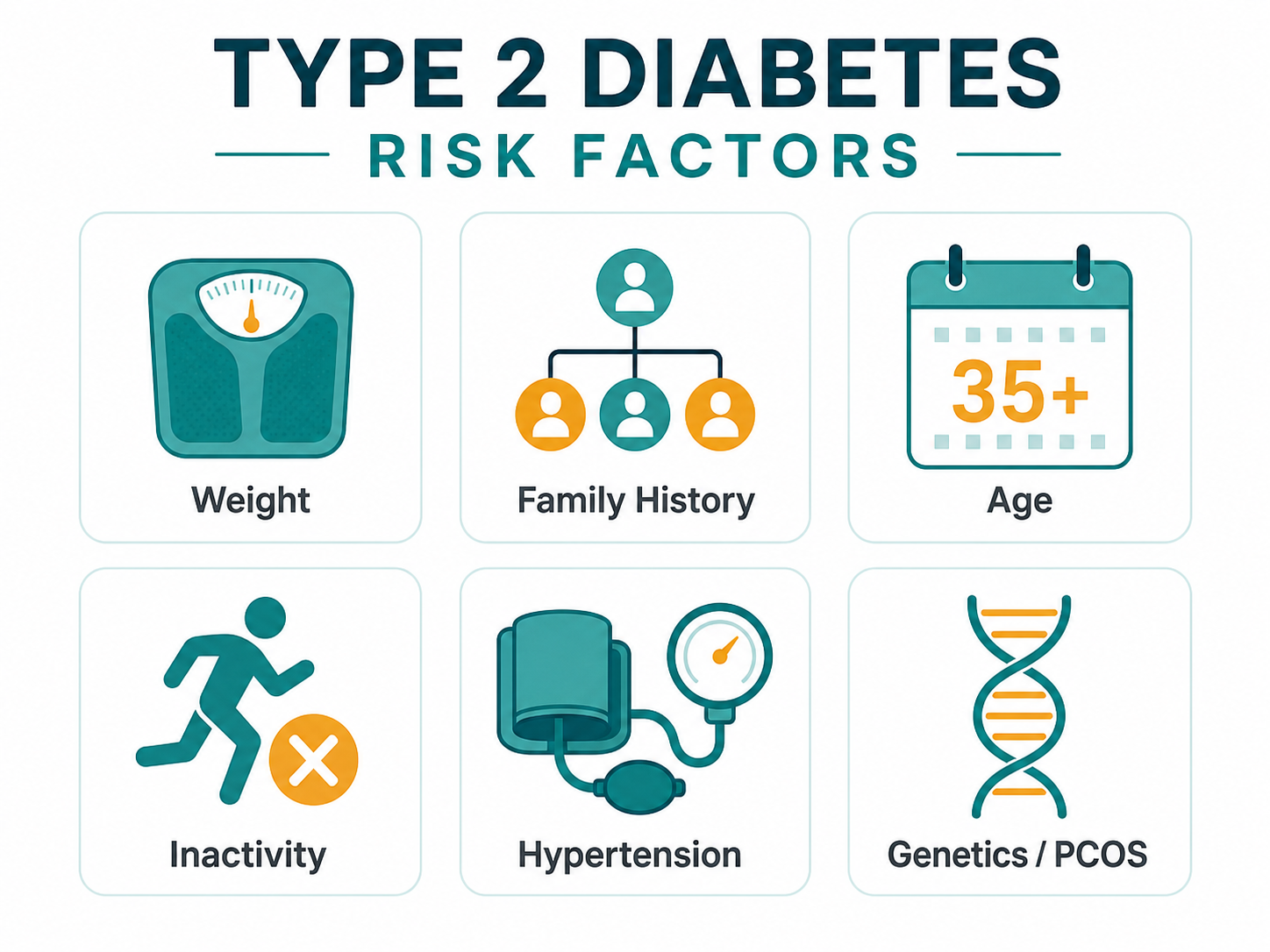
Major risk factors for Type 2 diabetes
- Overweight or obesity: Excess body weight, especially abdominal fat, is one of the strongest modifiable risk factors.
- Physical inactivity: A sedentary lifestyle reduces the body’s ability to use insulin efficiently.
- Family history: Having a parent or sibling with Type 2 diabetes significantly increases your risk.
- Age 35 or older: Risk increases with age, though Type 2 is now increasingly diagnosed in younger adults and teenagers.
- Ethnicity: African American, Hispanic/Latino, American Indian, Alaska Native, Asian American, and Pacific Islander individuals experience higher rates of Type 2 diabetes.
- History of gestational diabetes: A prior diagnosis of gestational diabetes or delivery of a baby weighing more than 9 pounds raises long-term Type 2 risk.
- High blood pressure: A blood pressure of 130/80 mm Hg or higher is associated with an increased risk of diabetes.
- Abnormal cholesterol or triglycerides: Low HDL (“good”) cholesterol or high triglycerides are associated with insulin resistance and increased risk of diabetes.
- Polycystic ovary syndrome (PCOS): PCOS is associated with insulin resistance and increases the risk of both prediabetes and Type 2 diabetes.
- Cardiovascular disease: A history of heart attack, stroke, or other cardiovascular disease is independently associated with increased diabetes risk.
Other factors that may contribute to risk include chronic stress and inadequate sleep, both of which are linked to hormonal and metabolic changes that can impair glucose regulation over time. These are not formal ADA screening criteria, but are worth discussing with your doctor as part of an overall health picture.
Should you be screened now? The ADA offers a free online diabetes risk test at diabetes.org/diabetes-risk-test. It takes less than two minutes and can indicate whether formal screening makes sense for you.
ADA 2026 screening guidance: All adults should begin screening at age 35. If you have overweight or obesity plus one or more risk factors, screening is recommended at any age. If results are normal, re-test at least every 3 years — or sooner if your risk profile changes.
What Is Prediabetes and Why Does It Matter?
Prediabetes means your blood sugar is higher than normal but not yet high enough to be diagnosed with diabetes. It affects an estimated 115 million American adults, and about 8 in 10 of them do not know they have it (CDC, 2026). Prediabetes is not just a warning sign — it carries its own health risks, including increased cardiovascular risk, and it significantly raises the likelihood of progressing to Type 2 diabetes if left unaddressed.
The good news is that prediabetes is among the most actionable conditions in medicine. The landmark Diabetes Prevention Program study showed that modest weight loss of 5–7% of body weight, combined with 150 minutes of moderate physical activity per week, reduced the risk of progression from prediabetes to Type 2 diabetes by 58% — and by 71% in adults over 60. These results have been replicated in real-world programs worldwide.
What should you do if you have prediabetes?
- Confirm the result: A single borderline test can vary day to day. Ask your doctor to repeat the test and discuss your full risk profile.
- Ask about the National Diabetes Prevention Program (NDPP): The CDC-recognized NDPP is a structured lifestyle program proven to reduce the risk of progression to Type 2 diabetes. It is covered by Medicare and many insurance plans. Find a local or online program at cdc.gov/diabetes/prevention.
- Focus on modest, sustainable changes: Losing 5–7% of your body weight — for a 200-pound person, that is 10–14 pounds — has been shown to meaningfully reduce risk.
- Get retested regularly: The ADA 2026 Standards recommend monitoring people with prediabetes for progression to diabetes at least annually, or more often based on individual risk.
How Is Diabetes Diagnosed? The Four Standard Tests
 Diabetes is confirmed with one of four blood tests, each measuring blood sugar in a different way. The ADA 2026 Standards confirm that the FPG, OGTT, A1c, and random glucose tests are all appropriate for diagnosis. In most cases, a positive result should be confirmed with a repeat test before a diagnosis is made — unless two different tests performed at the same time both meet the threshold, or symptoms leave little doubt.
Diabetes is confirmed with one of four blood tests, each measuring blood sugar in a different way. The ADA 2026 Standards confirm that the FPG, OGTT, A1c, and random glucose tests are all appropriate for diagnosis. In most cases, a positive result should be confirmed with a repeat test before a diagnosis is made — unless two different tests performed at the same time both meet the threshold, or symptoms leave little doubt.
1. Fasting Plasma Glucose (FPG) test
The FPG test measures your blood sugar after you have not eaten for at least 8 hours. It is usually done first thing in the morning. Because the pancreas continues to produce a small amount of insulin even during a fast, the test reveals how well your baseline blood sugar regulation is working.
- Normal: Below 100 mg/dL (5.6 mmol/L)
- Prediabetes: 100–125 mg/dL (5.6–6.9 mmol/L)
- Diabetes: 126 mg/dL (7.0 mmol/L) or higher
2. Oral Glucose Tolerance Test (OGTT)
The OGTT measures how your blood sugar responds to a glucose load. You fast for at least 8 hours, have a fasting blood draw, drink a standardized 75g glucose solution, and then have your blood sugar measured again two hours later. The ADA 2026 Standards note that adequate carbohydrate intake — at least 150g per day — should be maintained for the three days before the test to ensure accurate results.
- Normal: Below 140 mg/dL (7.8 mmol/L) at 2 hours
- Prediabetes: 140–199 mg/dL (7.8–11.0 mmol/L) at 2 hours
- Diabetes: 200 mg/dL (11.1 mmol/L) or higher at 2 hours
The OGTT is also commonly used during pregnancy to screen for gestational diabetes, though pregnancy-specific testing protocols differ from those used for general diabetes screening.
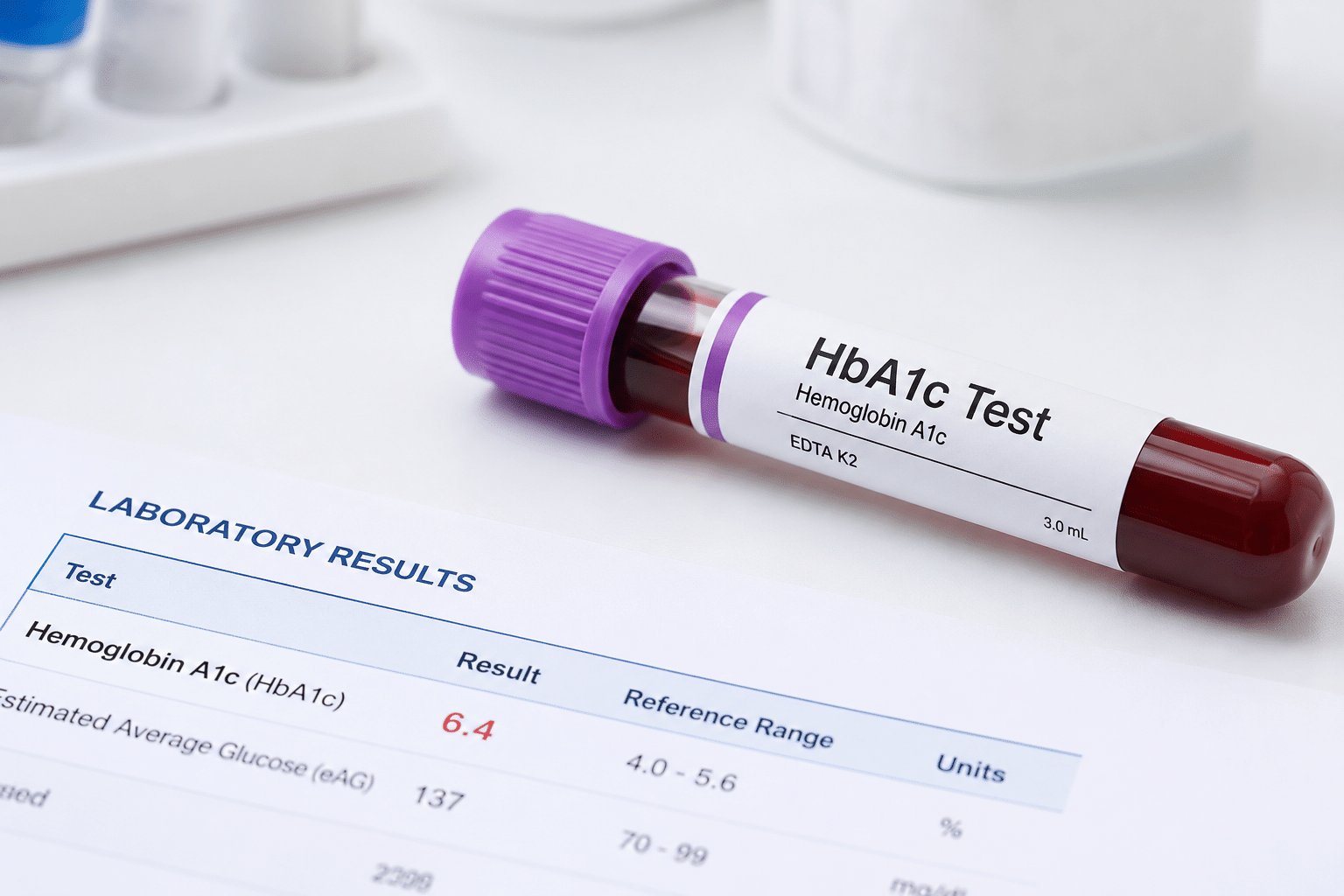
3. A1c test (HbA1c)
The A1c test measures the percentage of red blood cells with glucose attached. Because red blood cells live about 3 months — with the most recent weeks contributing more to the result than earlier ones — the A1c reflects your overall blood sugar trends over roughly the past 3 months. It does not require fasting and can be done at any time of day, making it a commonly used option in routine care.
- Normal: Below 5.7%
- Prediabetes: 5.7%–6.4%
- Diabetes: 6.5% or higher
As a practical reference: an A1c of 7% corresponds to an average blood sugar of about 154 mg/dL (8.6 mmol/L). An A1c of 6.5% corresponds to about 140 mg/dL (7.8 mmol/L).
When A1c may be less reliable: The A1c test can be less accurate in people with conditions that affect red blood cell turnover or hemoglobin structure — including sickle cell trait, hemolytic anemia, recent blood loss or transfusion, iron deficiency, and certain hemoglobin variants. If any of these apply to you, your doctor may rely more heavily on fasting glucose or OGTT results for diagnosis. Always inform your doctor about any blood or hemoglobin conditions before testing.
4. Random (non-fasting) glucose test
In someone with clear symptoms of diabetes — such as extreme thirst, frequent urination, and unexplained weight loss — a random blood sugar level of 200 mg/dL (11.1 mmol/L) or higher at any time of day is sufficient to confirm a diagnosis without a repeat test.
What if the type of diabetes is not clear at diagnosis?
Not every diagnosis fits neatly into Type 1 or Type 2, and classification can be uncertain at first. Adults with autoimmune diabetes — including LADA — are often initially mistaken for Type 2, especially if they are older and not severely underweight. When the clinical picture does not fit — for example, a person diagnosed with Type 2 who is not overweight, fails to respond to oral medications, or develops ketoacidosis — additional testing with an autoantibody panel (GAD65, IA-2, ZnT8) and a C-peptide test can clarify the diagnosis. See our full guide to types of diabetes for more on how different forms are distinguished.
What Should You Do After a Diabetes or Prediabetes Diagnosis?
Receiving a diabetes diagnosis brings a rush of new information. Here is a practical starting point for the first steps that matter most:
- Confirm your diabetes type: Type 1, Type 2, LADA, and other forms are managed differently. If there is any uncertainty about your type, ask about autoantibody testing and a C-peptide test. See our guide to types of diabetes.
- Start monitoring your blood sugar: Regular blood sugar testing is the foundation of diabetes management. Ask your doctor whether a glucose meter or a continuous glucose monitor (CGM) is appropriate for you.
- Build your care team: A primary care provider is a starting point, but most people with diabetes benefit from a broader team. Learn more about how to build your diabetes care team.
- Ask about a diabetes education program: The ADA recommends Diabetes Self-Management Education and Support (DSMES) at the time of diagnosis. Ask your doctor for a referral — DSMES is covered by most insurance plans and by Medicare.
- Review your eating pattern: No foods are completely off-limits, but understanding how carbohydrates affect your blood sugar is valuable from day one. Our diet and nutrition guide covers the major approaches.
Helpful Resources and Research
- ADA Standards of Care 2026 — Section 2: Diagnosis and Classification of Diabetes
- CDC National Diabetes Statistics Report, January 2026
- ADA Diabetes Risk Test (free, online)
- CDC National Diabetes Prevention Program — Find a Program
- TrialNet — Type 1 Diabetes Risk Screening
- NIDDK — Diabetes Overview and Diagnosis
Frequently Asked Questions
At what age should I be tested for diabetes?
The ADA 2026 Standards of Care recommend that all adults begin screening for prediabetes and Type 2 diabetes at age 35. If you are younger than 35 but have overweight or obesity and one or more additional risk factors — such as family history, high blood pressure, or a prior gestational diabetes diagnosis — screening should begin earlier. If results are normal, retesting is recommended at least every 3 years, or sooner if your risk profile changes.
What is the most common test used to diagnose diabetes?
The A1c test is commonly used because it does not require fasting and can be performed at any time of day. The fasting plasma glucose test and the oral glucose tolerance test are equally valid for diagnosis, and the choice often depends on the clinical situation. For example, the OGTT is preferred during pregnancy, and fasting glucose may be preferred when A1c could be unreliable due to a blood condition such as sickle cell trait.
What is the difference between prediabetes and diabetes?
Prediabetes means your blood sugar is above normal but not yet at the level that confirms a diabetes diagnosis. The prediabetes ranges are: fasting blood sugar of 100–125 mg/dL (5.6–6.9 mmol/L), a 2-hour OGTT result of 140–199 mg/dL (7.8–11.0 mmol/L), or an A1c of 5.7–6.4%. Prediabetes significantly raises the risk of progressing to Type 2 diabetes, but lifestyle changes — particularly modest weight loss and increased physical activity — can substantially reduce that risk.
Can diabetes be diagnosed from a single blood test?
In most cases, the ADA recommends confirming an abnormal result with a second test before making a diagnosis. The exception is when two different tests performed at the same visit both meet the threshold, or when a person has obvious symptoms of diabetes — extreme thirst, frequent urination, unexplained weight loss — alongside a random blood sugar of 200 mg/dL (11.1 mmol/L) or higher. A single borderline result without symptoms should always be confirmed before any diagnosis is made.
What does my A1c number mean?
An A1c below 5.7% is normal. An A1c of 5.7–6.4% indicates prediabetes. An A1c of 6.5% or higher on a confirmed test is diagnostic for diabetes. As a practical reference, an A1c of 7% corresponds to an average blood sugar of about 154 mg/dL (8.6 mmol/L) — a common treatment target for many adults with diabetes. Your personal A1c target may be set higher or lower by your care team based on age, risk of low blood sugar, and other factors.
My fasting blood sugar was 105 mg/dL. Should I be worried?
A fasting result of 105 mg/dL (5.8 mmol/L) falls within the prediabetes range and warrants discussion with your doctor, but it is not a diagnosis of diabetes. Results can vary slightly from day to day depending on when you last ate, slept, and stressed. Your doctor will likely recommend a repeat test and a broader assessment of your risk factors. The most constructive response is to treat it as a motivating signal to make lifestyle changes if you have not already done so.
What is the difference between the FPG test and the OGTT?
The Fasting Plasma Glucose (FPG) test measures your blood sugar after at least 8 hours without eating, giving a snapshot of your baseline glucose regulation. The Oral Glucose Tolerance Test (OGTT) goes further — it measures how your blood sugar responds to a 75g glucose drink over 2 hours, revealing how well your body manages a glucose load. The OGTT is more sensitive for detecting early problems, particularly after meals, but requires more time. Both are equally valid for diagnosis per the ADA 2026 Standards.
Can stress or illness affect my diabetes test results?
Yes. Illness, surgery, and significant physical or emotional stress can temporarily raise blood sugar, as can certain medications including corticosteroids, some antipsychotics, and thiazide diuretics. If your test was performed during a period of acute illness or major stress, your doctor may recommend repeating it after you have recovered. This is one reason a confirmed diabetes diagnosis typically requires two abnormal results unless symptoms are unambiguous.
Does Type 1 diabetes have risk factors the same way Type 2 does?
Type 1 has a distinct risk profile from Type 2. It is primarily an autoimmune condition, and the main identifiable risk factor is having a first-degree relative with Type 1 diabetes. Certain genetic markers — particularly in the HLA gene region — also increase risk. However, most people who develop Type 1 have no family history of it, suggesting that environmental triggers play a substantial role. There are currently no lifestyle changes known to prevent Type 1 diabetes.
When should I ask about antibody testing or a C-peptide test?
These tests are worth requesting if something about your diagnosis does not seem to fit — for example, if you were diagnosed with Type 2 as an adult but are not overweight, are not responding well to oral medications, experienced diabetic ketoacidosis, or have a strong family history of Type 1. An autoantibody panel and a C-peptide test can clarify whether you have autoimmune diabetes, such as LADA, rather than Type 2. They are most reliably interpreted before insulin treatment has begun.
Last Updated on May 13, 2026