Diabetes and stroke are closely connected, and having diabetes can raise your risk of a stroke by about 1.5–2× compared with someone without diabetes.
That sounds scary, but here’s the empowering part: many stroke risks are modifiable. When you protect your blood vessels—by improving blood sugar, blood pressure, cholesterol, and daily habits—you also protect your brain.
Searching for a specific answer? Jump to our Frequently Asked Questions for quick tips on lowering stroke risk with diabetes.
Direct answer: The best way to lower stroke risk with diabetes is a “4-number plan”:
- Blood sugar: aim for time-in-range and fewer highs/lows (typical targets include 80–130 mg/dL (4.4–7.2 mmol/L) before meals and <180 mg/dL (10.0 mmol/L) after meals—individualized with your clinician).
- Blood pressure: if safely attainable, target <130/80 mmHg (and in higher cardio/kidney risk, a systolic goal <120 mmHg may be encouraged).
- LDL (“bad”) cholesterol: for many higher-risk adults with diabetes, a common goal is <70 mg/dL (1.8 mmol/L) with statin therapy when indicated.
- Fast action: learn stroke warning signs (FAST) and call 911 immediately if symptoms appear.
| Your “Stroke-Protection” Target | Typical Goal (talk with your clinician) | Why it matters |
|---|---|---|
| Blood sugar | Often 80–130 mg/dL (4.4–7.2 mmol/L) before meals; <180 mg/dL (10.0 mmol/L) after meals | High glucose damages vessel lining and accelerates plaque/inflammation |
| Blood pressure | If safe: <130/80 mmHg (sometimes systolic <120 for higher risk) | Top driver of stroke risk—lowering BP reduces stroke events |
| LDL cholesterol | Higher-risk adults often target <70 mg/dL (1.8 mmol/L) with statins as appropriate | Lower LDL slows atherosclerosis (plaque) that can block brain blood flow |
| Smoking | Quit + avoid secondhand smoke | Smoking increases clot risk and damages vessels—quitting helps quickly |
How does diabetes increase stroke risk?
Diabetes raises stroke risk through several “stacking” effects on blood vessels:
- Atherosclerosis: Diabetes speeds plaque buildup and artery narrowing, which can reduce blood flow to the brain and cause an ischemic stroke (the most common type).
- Small-vessel disease: High glucose and high blood pressure can damage tiny brain vessels, raising risk for “silent” strokes and cognitive decline over time.
- Clot-prone blood chemistry: Insulin resistance and inflammation can increase clot formation and impair normal vessel function.
👉 Key Risk Factors (and why they matter):
- High blood sugar harms blood vessels, increasing inflammation and the risk of blood clots.
- Insulin resistance is associated with impaired circulation and increased vascular risk.
- High blood pressure and abnormal cholesterol commonly accompany diabetes and strongly raise stroke risk.
Clinical insight: Diabetes is a major contributor to cerebral small vessel disease and nearly doubles overall stroke risk in population research and expert reviews.
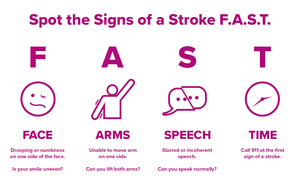
What are the FAST stroke warning signs (and what should I do)?
Stroke is a true emergency. If you notice symptoms, call 911 immediately—don’t drive yourself.
- F — Face drooping: One side droops or feels numb
- A — Arm weakness: One arm is weak or drifts downward
- S — Speech difficulty: Slurred speech or trouble speaking
- T — Time to call 911: Every minute matters
Tip: If you use a CGM, don’t get “stuck” checking glucose first. Treat stroke symptoms as an emergency. Paramedics can check glucose on arrival.
What complications are more common when diabetes and stroke overlap?
Diabetes and stroke can amplify each other’s impact. After a stroke, diabetes can make recovery harder—and after years of diabetes, the brain’s blood vessels may be more vulnerable.
Cerebral small vessel disease
Small-vessel disease can contribute to:
- Cognitive changes (slower thinking, reduced processing speed)
- Higher risk of vascular dementia over time
- “Silent” strokes seen on imaging (even without obvious symptoms)
Recurrent strokes
People with diabetes often carry more risk factors (blood pressure, cholesterol, kidney disease, inflammation), which can increase the chance of future strokes if those risks aren’t aggressively addressed.
Cardiovascular events
Stroke is part of a larger cardiovascular picture. Diabetes also raises the risk for heart attack, heart failure, and peripheral artery disease. The good news: improving the same “big levers” (BP, LDL, glucose, smoking, activity) helps protect both heart and brain.
Which medications may help lower stroke risk in type 2 diabetes?
Medication choices depend on your personal history (prior stroke, heart disease, kidney disease), your glucose patterns, cost/coverage, and side effects. But two medication classes come up often in 2026 guidance because they improve cardiovascular outcomes in the right patients.
GLP-1 receptor agonists (for example: semaglutide, dulaglutide, liraglutide)
- What the evidence suggests: Across large cardiovascular outcomes trials and meta-analyses, GLP-1 receptor agonists show a modest reduction in stroke or nonfatal stroke risk for many people with type 2 diabetes (the benefit varies by trial and population).
- Why they may help: They can improve weight, blood pressure, inflammation, and blood vessel function—factors that matter for stroke prevention.
- Bottom line: If you have type 2 diabetes and high cardiovascular risk, ask your clinician whether a GLP-1 RA with demonstrated cardiovascular benefit fits your plan.
SGLT2 inhibitors (for example: empagliflozin, dapagliflozin)
- What the evidence suggests: For stroke specifically, many analyses find SGLT2 inhibitors are neutral overall (not clearly lowering ischemic stroke risk), while providing strong benefits for heart failure and kidney protection.
- Why they still matter: Preventing heart failure and protecting kidneys can reduce overall cardiovascular stress and complications that raise stroke risk.
- Bottom line: If you have type 2 diabetes plus heart failure or chronic kidney disease, an SGLT2 inhibitor may be a key protective therapy.
Important: Aspirin is sometimes used after a prior stroke (secondary prevention), but for preventing a first stroke in people with diabetes, routine aspirin is not automatically recommended for everyone—this is a personalized decision with your clinician based on bleeding risk and cardiovascular risk.
What daily prevention steps make the biggest difference?

If you have diabetes, taking proactive measures can significantly reduce your risk of stroke. Think of this as your “brain protection checklist.”
Maintain optimal blood glucose (sugar) levels
- Typical targets for many non-pregnant adults include 80–130 mg/dL (4.4–7.2 mmol/L) before meals and <180 mg/dL (10.0 mmol/L) after meals, but your safest targets may differ based on age, medications, and hypoglycemia risk.
- If you use diabetes technology, a CGM can help you reduce time above range and avoid severe lows—both of which are important for vascular health.
- Ask about your A1C goal and your time-in-range goal if you wear a CGM.
Manage blood pressure and cholesterol
- Blood pressure: If it can be safely attained, an on-treatment goal of <130/80 mmHg is recommended; in people with higher cardiovascular or kidney risk, a systolic goal <120 mmHg may be encouraged.
- LDL cholesterol: For many higher-risk adults with diabetes, high-intensity statin therapy aims to reduce LDL by ≥50% and reach <70 mg/dL (1.8 mmol/L). If you’ve already had a stroke or have established ASCVD, your clinician may discuss even more aggressive LDL goals.
- If you’re prescribed a statin, consistency matters—statins lower stroke risk by reducing plaque progression and stabilizing existing plaque.
Adopt a heart- and brain-healthy lifestyle
- Exercise: Aim for about 150 minutes/week of moderate activity (or a plan you can sustain). If you’re new to activity, start small and build.
- Eating pattern: Mediterranean-style or DASH-style eating patterns support better blood pressure, cholesterol, and glucose.
- Sodium awareness: Lower sodium helps lower blood pressure, a major risk factor for stroke.
- Quit smoking: Smoking sharply increases stroke risk; quitting improves vessel health quickly and keeps improving over time.
- Sleep: Poor sleep and untreated sleep apnea can raise blood pressure and cardiovascular risk—ask if screening is right for you.
- Atrial fibrillation (AFib): An irregular heartbeat can cause clots that travel to the brain. If you have palpitations, shortness of breath, or unexplained fatigue, ask about screening.
- Kidney disease: Chronic kidney disease increases cardiovascular and stroke risk; kidney-protective therapy can be a major win.
- Medication lows (“sugar crashes”): Severe hypoglycemia can strain the heart and brain. If you’re having frequent lows, ask for a medication and dosing review.
Conclusion: what’s the most practical way to start today?
Understanding the diabetes–stroke connection helps you act earlier—and smarter. Start with the biggest levers (blood pressure, LDL cholesterol, and glucose patterns), learn FAST warning signs, and build a prevention plan you can actually live with.
🌟 Take charge of your health today! Bring this checklist to your next appointment and ask: “What are my BP, LDL, and glucose targets—and what’s the next best step to hit them safely?”
Helpful Resources & Research
- American Stroke Association: Stroke Symptoms (FAST)
- AHA/ASA 2024 Guideline: Primary Prevention of Stroke
- ADA: Standards of Care in Diabetes—2026 (overview)
- ADA Standards of Care—2026: Cardiovascular Disease & Risk Management (full text)
- ADA: Checking Your Blood Sugar (targets explained)
Frequently Asked Questions
Does diabetes really double your risk of stroke?
Yes—many studies show diabetes raises stroke risk about 1.5–2 times compared with people without diabetes. Risk increases with longer diabetes duration and when blood pressure, cholesterol, or smoking are also present.
What type of stroke is most linked to diabetes?
Diabetes is strongly linked to ischemic stroke (a clot blocking blood flow). It’s also associated with cerebral small vessel disease, which can lead to “silent” strokes and cognitive changes over time.
What blood sugar numbers best protect against stroke?
Targets are individualized, but many adults aim for about 80–130 mg/dL (4.4–7.2 mmol/L) before meals and under 180 mg/dL (10.0 mmol/L) after meals. The most protective strategy is reducing prolonged highs and avoiding severe lows—both strain the cardiovascular system.
What is the best blood pressure goal for people with diabetes to prevent stroke?
If it can be achieved safely, many people with diabetes target below 130/80 mmHg. If you have higher cardiovascular or kidney risk, your clinician may encourage an even lower systolic goal (under 120 mmHg), balancing benefits and side effects.
What LDL (“bad”) cholesterol level should I aim for if I have diabetes?
Many higher-risk adults with diabetes aim for LDL under 70 mg/dL (1.8 mmol/L) with statin therapy when appropriate. If you’ve already had a stroke or have established ASCVD, your clinician may discuss more aggressive LDL lowering.
Do GLP-1 medications like semaglutide help prevent stroke?
GLP-1 receptor agonists have cardiovascular benefits in many people with type 2 diabetes, and meta-analyses suggest a modest reduction in stroke/nonfatal stroke risk in some populations. Whether it’s right for you depends on your history, kidney function, weight goals, and coverage.
Do SGLT2 inhibitors like empagliflozin lower stroke risk?
For stroke specifically, many studies show a neutral overall effect, but SGLT2 inhibitors strongly reduce heart failure hospitalization and protect kidney function—two big wins that lower overall cardiovascular risk.
Should everyone with diabetes take aspirin to prevent a first stroke?
Not necessarily. For people with diabetes who have never had a stroke or heart attack, routine aspirin for first-stroke prevention is not automatically recommended because bleeding risk may outweigh benefit. This decision should be individualized with your clinician.
What are the FAST signs of stroke again?
F = Face drooping, A = Arm weakness, S = Speech difficulty, T = Time to call 911. If you suspect stroke, call 911 immediately—do not wait.
What’s the single most effective “starter step” to lower stroke risk with diabetes?
If you can only focus on one thing this month: get serious about blood pressure (home checks + treatment adherence) and LDL cholesterol (statin adherence if prescribed). Those two changes often deliver the biggest stroke-risk reduction, especially when combined with steadier glucose patterns.
Last Updated on February 12, 2026
