COVID-19 and diabetes are a dangerous combination — and understanding why can help you stay safer, manage your blood sugar more confidently, and know exactly what to do if you get sick. People with Type 1 or Type 2 diabetes face a significantly higher risk of serious illness from COVID-19, and the virus itself can create new blood sugar challenges even in people who had things well under control before infection.
This article discusses what makes COVID-19 especially dangerous when diabetes is involved, how to control your blood sugar during an active infection, what we now know about new-onset diabetes after COVID-19, and the latest vaccine recommendations. Whether you were recently diagnosed or have been managing diabetes for years, you’ll find practical, evidence-based information here.
Looking for a quick answer? Scroll down to our Frequently Asked Questions section for fast info about COVID-19 and diabetes.
Quick Reference: COVID-19 Risk and Diabetes at a Glance
- People with diabetes are at a greater risk of hospitalization and serious illness from COVID-19.
- Poor blood sugar control is linked to worse COVID-19 outcomes — risk increases gradually with higher glucose levels and other health issues.
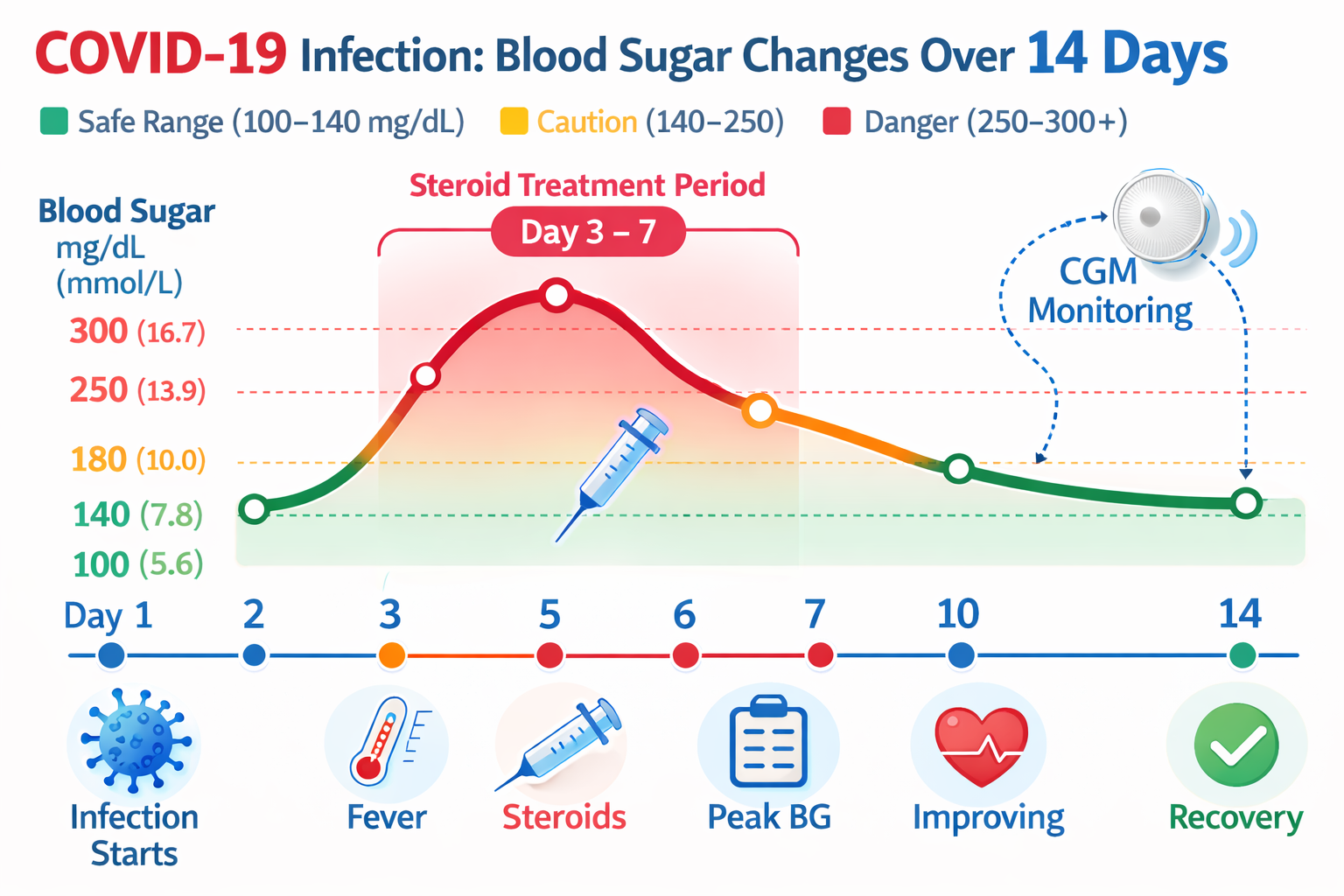
- Steroids used to treat COVID, like dexamethasone, can significantly raise blood sugar.
- COVID-19 has been linked to new-onset diabetes in some individuals, including those with no previous history.
- COVID-19 vaccination is generally beneficial for adults with diabetes — discuss timing and current formulations with your provider.
- A CGM is the most effective tool for tracking rapidly fluctuating blood sugar levels during infection.
- Insulin remains the most reliable method for managing blood sugar during serious illness.
- (See Pumping Insulin, 7th Edition, and Using Insulin for full sick-day management guidance.)
Why does COVID-19 hit harder when you have diabetes?
High blood sugar, excess weight, high blood pressure, and cardiovascular disease all promote ongoing inflammation and oxidation in the body. This environment weakens your immune system even before the virus arrives. When COVID-19 enters the picture, it greatly increases that inflammation, often pushing it to dangerous levels.
Higher blood sugar also hampers oxygen delivery through blood vessels already damaged by years of high glucose levels. This explains why breathing problems are often more severe in people with diabetes. When the virus attacks, lungs with fragile, leaky blood vessels struggle to absorb oxygen normally.
How COVID-19 enters cells — and why diabetes makes it worse
COVID-19 enters your cells through a receptor called ACE2 (angiotensin-converting enzyme 2), which is located on the surface of cells in your nose, mouth, lungs, heart, kidneys, intestines, and nervous system. Because ACE2 exists in many organs, the virus can cause damage in multiple areas at once — not just the lungs.
Researchers are investigating whether diabetes alters ACE2 expression in ways that could worsen COVID-19 infection, and this remains an active area of research. ACE2 biology is complex and varies by tissue type, leading to mixed findings. What is clearer is that the broader metabolic and vascular problems associated with diabetes — such as chronic inflammation, impaired immune responses, damaged blood vessels, and insulin resistance — create a much more difficult environment for the body to combat serious infections. ACE2 is part of this picture, but not the whole story.
The inflammatory double hit
Your body relies on two pathways to regulate blood pressure and inflammation. Think of them as a gas pedal (the ACE pathway, which increases blood pressure and inflammation) and a brake (the ACE2 pathway, which decreases them).
Diabetes and its common companions — excess weight, kidney disease, heart disease — already press your foot down on the gas pedal. COVID-19 then hits the brakes by attaching to ACE2 receptors, disabling the anti-inflammatory pathway. The result is a dangerous spike in blood pressure, inflammation, and clotting that can quickly become life-threatening.
The table below highlights risk factors that worsen COVID-19 outcomes in people with diabetes.
| Risk Factor | How It Worsens COVID-19 | What You Can Do |
|---|---|---|
| Poorer blood sugar control | Weakens immune response; promotes ongoing inflammation and vascular damage | Improve glucose control; use CGM during illness |
| Excess weight | Increases inflammation; worsens breathing | Even modest weight loss reduces risk |
| High blood pressure | Already activates inflammatory pathways | Stay on your BP medications (see ACE/ARB section below) |
| Cardiovascular disease | Heart needs more oxygen during infection | Contact your provider early if symptoms appear |
| Kidney disease (high microalbumin) | Signals leaky blood vessels in lungs | Monitor closely; early treatment is key |
How do you manage blood sugar during an active COVID-19 infection?
An active infection is one of the most difficult blood sugar situations you will encounter. Multiple factors come into play simultaneously to raise your glucose levels, and they can increase quickly.
Why does your blood sugar spike when you’re sick?
When your body fights any infection, it releases stress hormones like cortisol and adrenaline. These hormones signal your liver to release extra glucose for energy, which raises your blood sugar even if you are not eating. This is your body’s natural emergency response, but with diabetes, it can cause readings to become dangerously high.
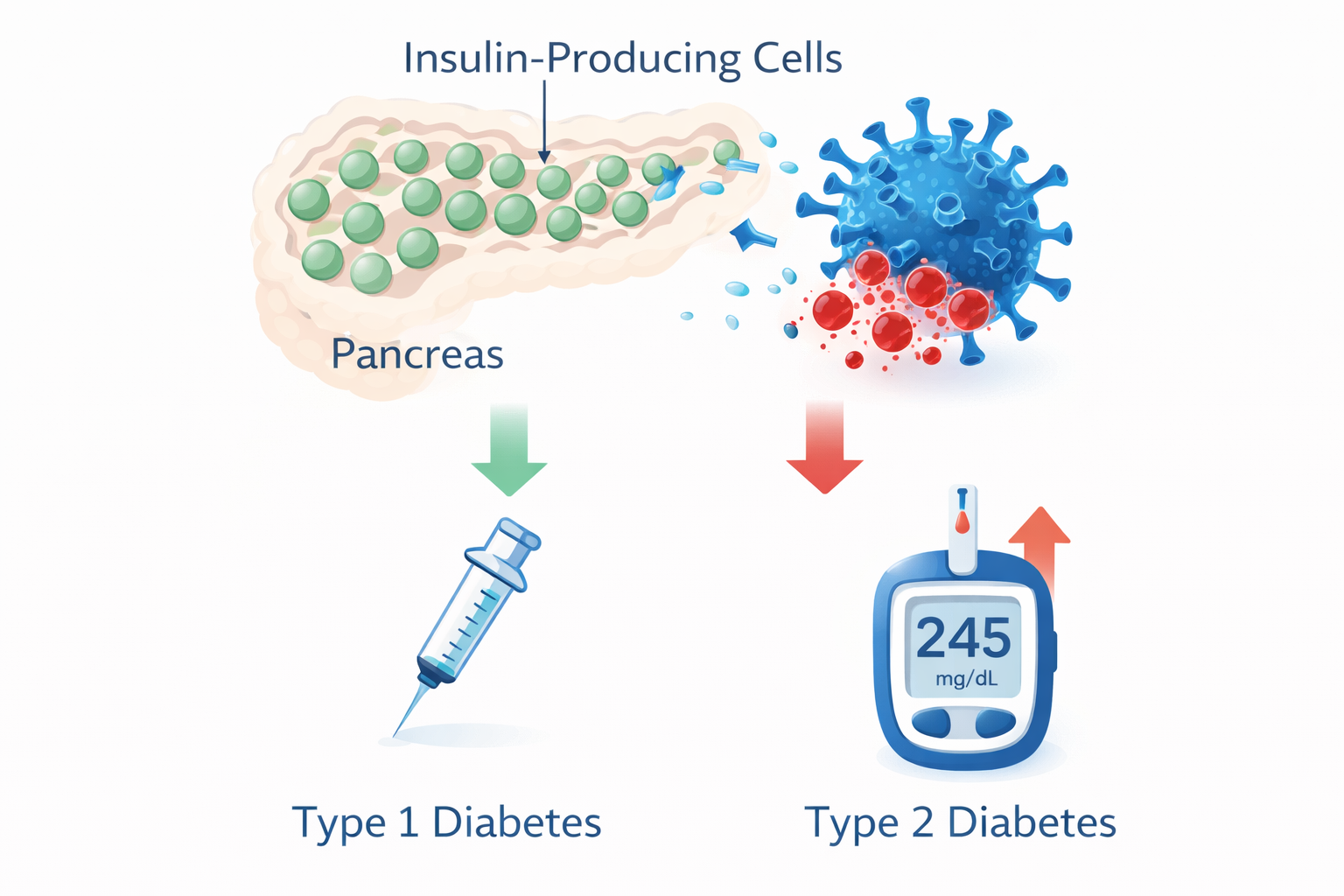
COVID-19 has an additional effect that most viruses do not: it can directly harm the insulin-producing cells in your pancreas, decreasing your natural insulin production. This is one reason why some people with Type 2 diabetes who previously managed without insulin might temporarily need it during a serious COVID infection.
Steroids and blood sugar: a crucial warning
Dexamethasone and other steroids are often prescribed for moderate to severe COVID-19. They effectively reduce the dangerous cytokine storm (more on that below), but they come with a significant side effect: they can cause sharp, rapid increases in blood sugar, often pushing readings above 300 mg/dL (16.7 mmol/L) within hours of a dose.
If you are prescribed steroids and have diabetes, contact your diabetes care team immediately. Your insulin doses may need to increase significantly, and you will need to monitor your blood sugar more frequently — often every 2 to 4 hours. A continuous glucose monitor (CGM) is especially helpful during this period, as it provides real-time readings and alerts you to rapid changes.
Sick-day blood sugar goals
Sick-Day Blood Sugar Guidelines (COVID-19 or Any Infection)
- Check blood sugar every 2–4 hours (or use a CGM with alerts).
- General illness target: 140–180 mg/dL (7.8–10.0 mmol/L) is a common inpatient goal — your personal target may differ, especially if you use insulin or a pump. Ask your provider what range is right for you.
- Note: People on insulin, particularly those with Type 1 diabetes, also face hypoglycemia risk during illness if appetite is reduced — do not over-correct without monitoring.
- Alert level: Contact your provider if readings stay above 240 mg/dL (13.3 mmol/L) for more than 2 checks.
- Danger zone: Seek emergency care if readings exceed 300 mg/dL (16.7 mmol/L) or you develop nausea or vomiting.
- Type 1 diabetes: Check ketones if blood sugar is above 240 mg/dL (13.3 mmol/L).
- Stay hydrated: Dehydration raises blood sugar and worsens kidney stress.
- Never stop insulin entirely, even if you are not eating.
For detailed guidance on adjusting insulin doses during illness, consult Pumping Insulin, 7th Edition. The Insulin Dose Guide also offers step-by-step guidance for adjustments.
How the cytokine storm impacts blood sugar
The immune system’s initial response to COVID-19 involves releasing proteins called cytokines, which cause inflammation to fight the virus. This is a normal and necessary reaction. The issue arises when the release becomes too intense — known as a cytokine storm — before the body’s more targeted antibody response can develop (antibodies take 10 to 14 days to fully form).
COVID-19 is especially effective at worsening cytokine storms: it delays the body’s production of anti-inflammatory interferons while actively encouraging more inflammation. An uncontrolled cytokine storm can damage organs, fill the lungs with fluid, and cause the breathing difficulties that require ICU care. For people with diabetes, who already have elevated baseline inflammation, this escalation can occur more quickly.
Dexamethasone significantly lessens cytokine storm severity and has been shown to decrease mortality in severe COVID-19 cases — but keep in mind the blood sugar trade-off described above.
Can COVID-19 cause new diabetes or worsen existing diabetes?
Research published since 2021 has shown that COVID-19 infection is linked to a higher risk of new diabetes diagnoses in the months after infection. This is a significant and genuine finding — but the full picture is more complex than early reports indicated, and researchers continue working to understand it.
What we know about diabetes after COVID
Several large studies have found that people who had COVID-19 are more likely to receive a new diagnosis of diabetes in the months following infection compared to those who did not have COVID-19. The increased risk seems higher after more severe infections.
The underlying mechanisms are likely complex and still under investigation. Possible factors include: the direct impact of the virus on insulin-producing cells in the pancreas, broader inflammatory and immune responses, stress-induced hyperglycemia (blood sugar increases caused by severe illness stress), steroid treatment during hospitalization, and the unmasking of pre-existing prediabetes or undiagnosed diabetes that the illness revealed. It is probably not one single cause but a combination of factors that vary from person to person.
Early reports characterized some post-COVID cases as “Type 1-like” or “Type 2-like,” but these labels have proven difficult to apply consistently in practice. Many post-COVID cases do not fit clearly into either category. Not everyone who develops blood sugar issues after COVID-19 will have permanent diabetes — some cases seem to improve over time. What matters most to you is not the label but whether your blood sugar is functioning normally after the infection.
Warning signs of new-onset diabetes following COVID-19
Watch for these symptoms in the weeks and months following COVID-19 infection:
- Unusual thirst or dry mouth.
- Urinating more frequently than usual, including during the night.
- Unexplained weight loss.
- Severe fatigue that doesn’t get better with rest.
- Blurred vision.
- Slow-healing cuts or infections.
If you notice any of these symptoms after COVID-19, ask your doctor for a fasting blood sugar or A1c test. Detecting new-onset diabetes early makes management much simpler.
What if you already have diabetes?
If you already have diabetes and contract COVID-19, expect your blood sugar to be more difficult to control than usual. The stress response from the infection, direct effects on the pancreas, and possible steroid treatment can all cause readings to rise. People who previously managed with oral medications might temporarily need insulin.
Once you recover from COVID-19, your blood sugar levels may go back to normal — or you might need to make some adjustments. Work with your healthcare team to revisit your treatment plan in the weeks after recovering.
Should you continue taking blood pressure medications like ACE inhibitors or ARBs?
Yes. If you take ACE inhibitors (such as lisinopril or enalapril) or ARBs (such as losartan) for blood pressure, heart failure, or kidney protection, you should continue taking them unless your doctor specifically tells you to stop.
Early in the pandemic, there was concern that these medications might increase ACE2 receptors and allow more virus to enter cells. More recent research has consistently shown that these medications appear to be protective rather than harmful in COVID-19. Both major diabetes and cardiology organizations recommend continuing these medications during COVID-19 infection. Do not stop them on your own.
What should you do if you have high blood pressure or heart disease along with diabetes?
High blood pressure and heart disease are more common in people with diabetes, and they increase the risk during COVID-19. COVID-19 is mainly a viral infection, but bacterial superinfection can occur, especially in hospitalized patients or those on long-term ventilators, which can put extra stress on the heart as oxygen delivery decreases. Fever also raises the heart rate and can cause arrhythmias (irregular heartbeats).
Cardiologist Dr. Eric Adler from the University of California, San Diego, emphasizes that people with existing heart issues need more oxygen at baseline — and when a virus like COVID-19 attacks the lungs, the gap between what the heart needs and what the lungs can deliver widens dangerously, increasing the risk of stroke.
Five steps if you have high blood pressure or heart disease
- Prioritize your safety first. Follow all current prevention guidelines: stay up to date on vaccines, wear a mask in high-risk settings, and avoid crowded indoor spaces during periods of high transmission.
- Contact your healthcare provider right away if you experience symptoms — fever, shortness of breath, a new cough, or chest discomfort.
- Continue taking your medications. Do not stop your blood pressure, heart, or diabetes medicines without consulting your doctor.
- Listen to your body. Do not ignore chest pain or tightness, numbness, confusion, or unusual shortness of breath. These can be signs of a heart attack or stroke, even during a COVID infection.
- Eat well and stay active. A balanced diet and at least 30 minutes of daily exercise support your immune system and heart health, even when you’re feeling under the weather.
Are COVID-19 vaccines advised for people with diabetes?
For most adults with diabetes, the benefits of COVID-19 vaccination far outweigh the risks, and vaccination is generally recommended by the American Diabetes Association (ADA) and other major health organizations. Diabetes is recognized as a risk factor for severe COVID-19, which is why people with diabetes are consistently identified as a group for whom vaccination provides significant protection.
Although the current CDC guidance (2025–2026) has shifted toward shared clinical decision-making for many age groups, the universal strong recommendation language used earlier in the pandemic is more appropriate for diabetes. If you have not discussed your COVID vaccination status with your provider recently, it is worth raising at your next visit.
Do COVID vaccines impact blood sugar levels?
Most people with diabetes do not experience any significant blood sugar changes after COVID vaccination. Some may notice a slight, temporary rise in blood sugar within 24 to 48 hours following a dose — similar to what can happen after any vaccine or minor illness. This is usually a normal immune response (mild inflammation) and tends to resolve quickly.
Here are some helpful tips for vaccine day:
- Check your blood sugar more often in the 24–48 hours after your vaccine (or rely on CGM alerts if you use one).
- Stay well-hydrated.
- If you develop a mild fever after vaccination, this can temporarily raise blood sugar — treat the fever as you normally would.
- A sore arm or fatigue after vaccination is normal and should not lead you to change your diabetes medications.
Which COVID vaccines are available now? (2026 update)
Visit CDC.gov for a clear list of available vaccines.
What are the considerations for managing Long COVID and diabetes?
Long COVID — symptoms persisting for weeks or months after infection — can cause ongoing difficulties in managing blood sugar. Research also suggests that vaccination reduces the likelihood of developing Long COVID. Fatigue, decreased appetite, and activity restrictions can disrupt daily routines. Some people with Long COVID also experience new or worsened blood sugar swings that are not related to diet or medication changes.
If you are experiencing Long COVID symptoms and notice your blood sugar control has become less predictable, discuss this with your healthcare team. A continuous glucose monitor (CGM) can be especially helpful during recovery, providing detailed data to share with your doctor and helping you identify patterns that would be invisible with fingerstick testing alone.
What additional steps can you take to reduce your COVID-19 risk with diabetes?
The most important step you can take is managing your blood sugar. Good glucose control is linked to better outcomes if you contract COVID-19 — and the evidence clearly shows that worsening blood sugar levels and other health issues like high blood pressure and excess weight increase that risk. In addition, several practical steps are especially helpful when you have diabetes:
- Aim for the best blood sugar control you can achieve — progress along a continuum matters, and every step toward better control is valuable.
- Use a CGM if available: it is the most effective way to detect and respond to quick blood sugar changes during illness.
- Stay current on recommended vaccines: flu, pneumonia, shingles, and updated COVID-19 vaccines all help reduce your overall risk of infection — if in doubt, discuss COVID vaccination with your provider.
- Manage your exposure carefully: indoor crowded spaces pose a higher risk than outdoor activities.
- Contact your healthcare team promptly at the first sign of COVID-19 symptoms — antiviral treatments are most effective when started within the first few days.
- Address modifiable risk factors along with diabetes: managing blood pressure, maintaining a healthy weight, and exercising regularly all support your immune system.
Helpful Resources & Research
The following resources offer more detailed information on COVID-19 and diabetes:
- ADA Standards of Care 2026: Section 4 (Comprehensive Medical Evaluation)
- CDC: COVID-19 and People with Certain Medical Conditions
- FDA: COVID-19 Vaccines and Related Updates
- For emerging evidence on COVID-19 and new-onset diabetes, search “COVID-19 new onset diabetes” in PubMed for peer-reviewed studies.
Frequently Asked Questions: COVID-19 and Diabetes
Why is COVID-19 more dangerous for people with diabetes?
People with diabetes often experience ongoing inflammation, weakened immune responses, and blood vessel damage that COVID-19 can quickly worsen. Diabetes-related metabolic and vascular issues make it harder for the body to control the infection and recover from organ stress. Other factors like high blood pressure, excess weight, and kidney disease — which are more common with diabetes — increase the risk even more.
How does COVID-19 affect blood sugar levels?
COVID-19 triggers a stress response that releases hormones, causing your blood sugar to rise, even if you are not eating. The virus can also directly damage insulin-producing cells in the pancreas, reducing your natural insulin supply. If your doctor prescribes steroids to treat the infection, these can spike blood sugar dramatically — sometimes above 300 mg/dL (16.7 mmol/L) — requiring rapid insulin dose adjustments.
What blood sugar level is considered dangerous during a COVID-19 infection?
During illness, a common inpatient guideline is a blood sugar range of 140–180 mg/dL (7.8–10.0 mmol/L), but your personal target may vary — especially if you use insulin, since hypoglycemia from reduced appetite is also a real concern. Contact your healthcare provider if blood sugar remains above 240 mg/dL (13.3 mmol/L) after two consecutive checks. Seek emergency care if readings exceed 300 mg/dL (16.7 mmol/L) or if you experience nausea, vomiting, or difficulty breathing. People with Type 1 or Type 2 diabetes should also check for ketones when blood sugar goes above 240 mg/dL (13.3 mmol/L).
Can COVID-19 cause diabetes in someone who has never had it before?
Research has found that people who had COVID-19 are more likely to receive a new diabetes diagnosis in the months after infection compared to those who were not infected. The reasons are probably complex — possible factors include effects on insulin-producing cells, inflammation, stress-induced high blood sugar during severe illness, and steroid treatment. Not everyone who develops blood sugar issues after COVID will develop permanent diabetes. If you notice increased thirst, frequent urination, or unexplained weight loss after infection, ask your doctor for a blood sugar test.
Should I continue taking my ACE inhibitor or ARB medication if I get COVID-19?
Yes. Despite initial concerns, research consistently shows that ACE inhibitors (like lisinopril) and ARBs (like losartan) are protective rather than harmful during COVID-19. Both the ADA and major cardiology organizations recommend continuing these medications. Never stop them without consulting your doctor first.
Are COVID-19 vaccines recommended for people with diabetes?
For most adults with diabetes, the advantages of COVID-19 vaccination far outweigh the risks. Diabetes is a recognized risk factor for severe COVID-19, and updated vaccines provide significant protection against illness or more serious complications. A COVID vaccine is your most important safeguard against hospitalization and death. If you have questions, talk with your healthcare provider about timing and available vaccine options. The effect of vaccination on blood sugar levels is minimal for most people.
Can COVID vaccines cause a blood sugar spike?
A small, temporary increase in blood sugar can occur within 24–48 hours after receiving a COVID vaccine, similar to reactions seen with other vaccines or minor illnesses. This increase is usually mild and goes away on its own. Check your blood sugar more often than usual after your vaccine and manage any fever normally. Contact your provider if your levels remain high for more than 48 hours.
What is a cytokine storm, and why does it matter in relation to diabetes?
Cytokines are inflammatory proteins that your immune system uses to fight infections, but they can also increase resistance to insulin. A cytokine storm happens when this response becomes too intense and starts damaging your own tissues — especially the lungs. People with diabetes already have higher baseline inflammation, which means their immune response can escalate more quickly and severely, making cytokine storms more likely and more dangerous.
How can I use a CGM while I have a COVID-19 infection?
A continuous glucose monitor (CGM) is one of the most useful tools you can have during a COVID infection. It provides real-time blood sugar readings every few minutes and alerts you to rapid increases or decreases, allowing you to adjust your insulin without frequent fingerstick tests while you are feeling unwell. This is especially important if steroids are prescribed, as glucose can spike very quickly.
What should I do if I get COVID-19 and have diabetes?
Contact your healthcare provider as soon as you test positive — antiviral treatments work best when started within the first 5 days of symptoms. Monitor your blood sugar every 2–4 hours (or use your CGM with alerts set). Stay hydrated, never stop your insulin, and watch for warning signs like blood sugar above 240 mg/dL (13.3 mmol/L) or ketones. Have a plan ready for who to call if you deteriorate quickly.
Last Updated on March 25, 2026