 Supplements for diabetic retinopathy are increasingly popular — but the science behind them is more complex than most product labels suggest. If you have diabetic retinopathy (DR) or diabetic macular edema (DME), you may have heard that certain vitamins, antioxidants, or herbs can lower VEGF — the protein that drives abnormal blood vessel growth in your eye — and protect your vision. Some of that research is promising. But much of it is early, small, or limited to lab studies — not solid proof.
Supplements for diabetic retinopathy are increasingly popular — but the science behind them is more complex than most product labels suggest. If you have diabetic retinopathy (DR) or diabetic macular edema (DME), you may have heard that certain vitamins, antioxidants, or herbs can lower VEGF — the protein that drives abnormal blood vessel growth in your eye — and protect your vision. Some of that research is promising. But much of it is early, small, or limited to lab studies — not solid proof.
This article breaks down the current evidence on seven commonly discussed supplements, ranks them by the strength and practicality of the human research, and tells you what your eye doctor would want you to know before adding anything to your routine.
⚠️ Bottom Line First
No supplement has been proven to replace anti-VEGF injections for center-involved diabetic macular edema. The most relevant evidence supports correcting vitamin D deficiency alongside standard treatment. Other supplements may offer supportive benefits but should not delay proven eye care.
↓ Jump to Frequently Asked Questions
What Is VEGF, and Why Does It Matter for Diabetic Eye Disease?
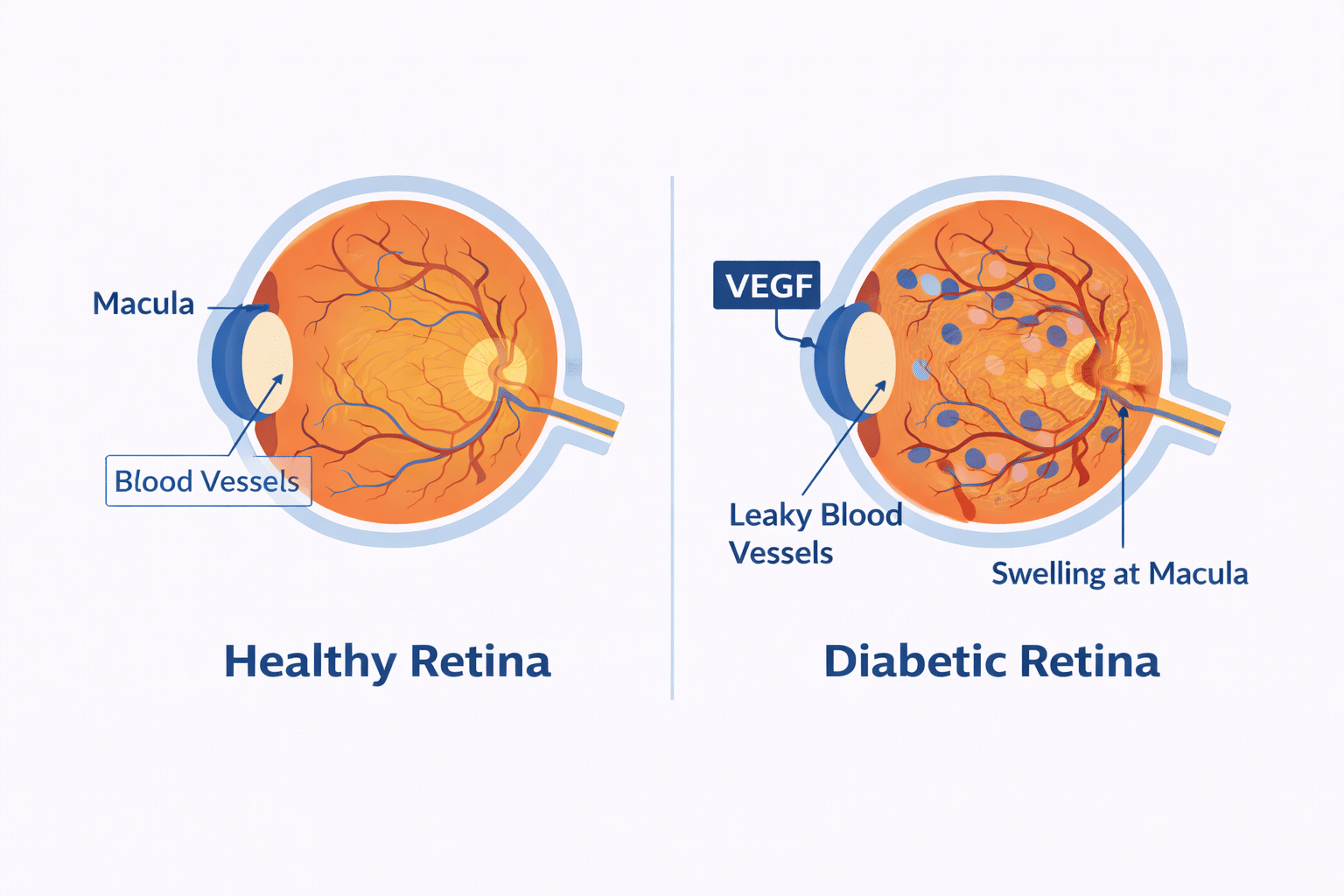
VEGF stands for vascular endothelial growth factor — a protein your body produces to grow new blood vessels. In healthy amounts, VEGF is beneficial. But in people with diabetes, high blood sugar damages the tiny blood vessels in the retina (the light-sensitive layer at the back of your eye). In response, the body floods the eye with VEGF, triggering the growth of abnormal, leaky vessels. This can lead to:
- Diabetic retinopathy (DR) — damage to retinal blood vessels over time.
- Diabetic macular edema (DME) — a buildup of fluid in the macula, the part of your eye responsible for sharp central vision.
 Anti-VEGF injections (such as bevacizumab, ranibizumab, and aflibercept) block this process directly in the eye and are the gold-standard treatment for center-involved DME. The key question is: can supplements reduce VEGF systemically — and does that actually help your retina?
Anti-VEGF injections (such as bevacizumab, ranibizumab, and aflibercept) block this process directly in the eye and are the gold-standard treatment for center-involved DME. The key question is: can supplements reduce VEGF systemically — and does that actually help your retina?
The honest answer: lowering VEGF in your bloodstream is not the same as lowering VEGF activity in your eye. A supplement can alter a blood test result without meaningfully reducing retinal swelling or protecting your vision. That distinction shapes everything below.
Supplement Evidence at a Glance
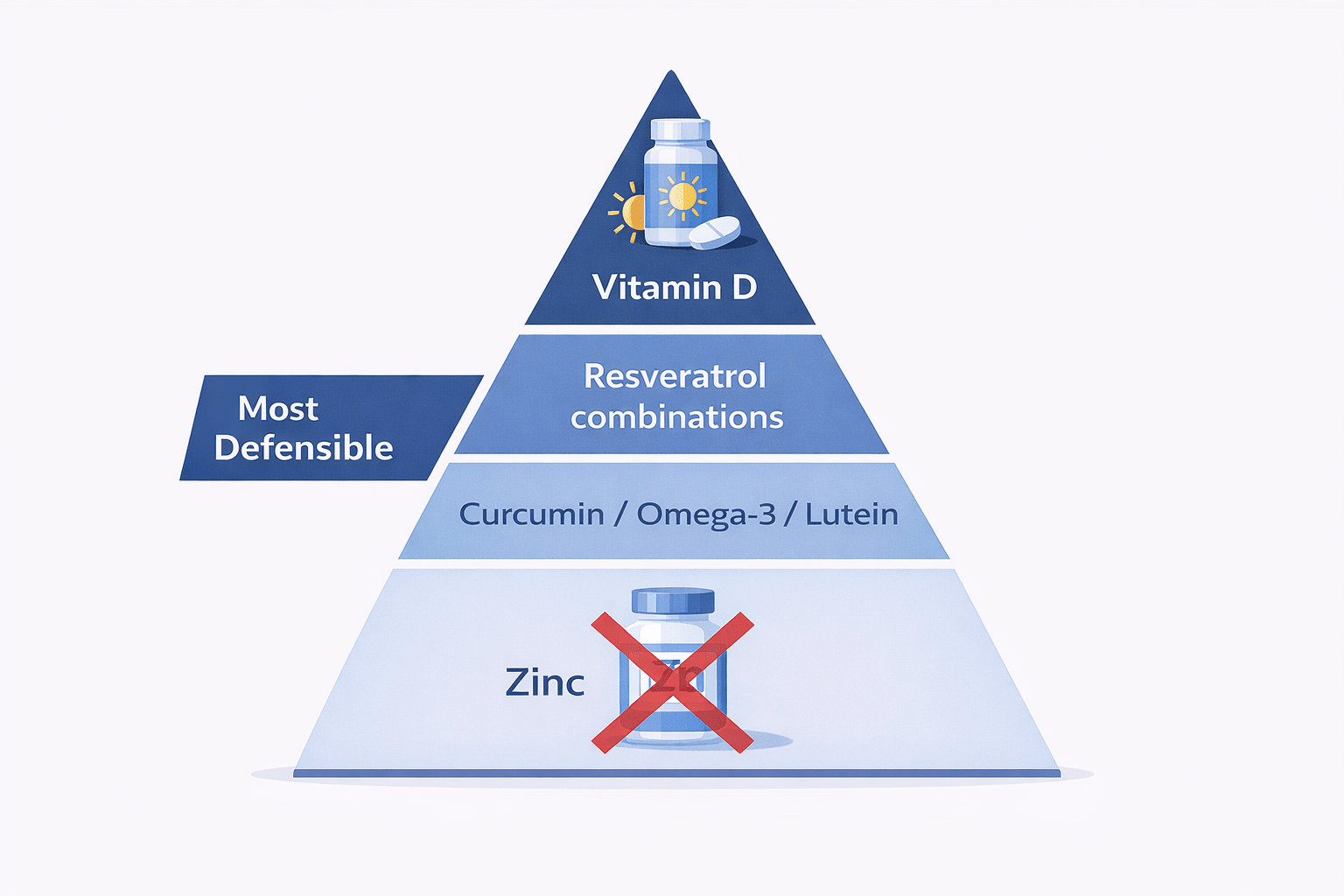
A quick-reference overview of seven supplements, ranked from most to least supported by clinical evidence for diabetic eye disease:
| Supplement | Best Evidence Type | Main Finding | Strength |
|---|---|---|---|
| Vitamin D | Randomized clinical trial (DME) | Repletion of deficiency may improve response to bevacizumab | Moderate (adjunct) |
| Resveratrol combination | Prospective comparative study | Fewer injections, greater thickness reduction vs. injections alone | Low–Moderate |
| Curcumin | Small randomized trial (oxidative markers) | Promising early signal; not proven for retinal edema | Low |
| Omega-3 fatty acids | Observational + mixed RCTs | General metabolic support; not a VEGF-lowering therapy | Low |
| Lutein / Zeaxanthin | Small clinical studies | Antioxidant / visual function support; no direct VEGF effect | Low |
| Crocin (saffron) | Placebo-controlled RCT (diabetic maculopathy) | Interesting early signal; still investigational | Low |
| Zinc | Randomized controlled trial (DR) | Did not lower serum VEGF in diabetic retinopathy patients | Negative evidence |
Detailed Evidence Breakdown
The tables below expand on study design, dosing, VEGF effects, and retinal outcomes. Because this data spans six variables, it is presented across two companion tables for mobile readability.
Note: Strength of evidence reflects current human clinical support, not mechanistic plausibility. Most data are adjunctive and should not be presented as replacements for anti-VEGF retinal therapy.
Table A — Study Type, Dose & Strength of Evidence
| Supplement | Study Type | Dose / Regimen | Strength of Evidence |
|---|---|---|---|
| Vitamin D | Randomized adjunct study in DME; separate human biomarker data | Deficiency correction; regimen varied by study | Moderate for deficiency correction; low for direct anti-VEGF retinal claim |
| Resveratrol formulations | Prospective comparative adjunct study in DME | Combination supplement; formulation-specific | Low–Moderate |
| Curcumin | Small clinical studies + randomized data; strong preclinical rationale | Formulation-dependent; bioavailability is a major issue | Low to Moderate |
| Omega-3 fatty acids | Observational studies + randomized placebo-controlled trial | DHA/EPA regimens varied by study | Low |
| Lutein / Zeaxanthin | Small human supplementation studies in NPDR | Varied by study | Low |
| Crocin / saffron | Placebo-controlled randomized clinical trial in diabetic maculopathy | Study-specific crocin regimen | Low to Moderate |
| Zinc | Randomized controlled study in DR | Study-specific oral zinc regimen | Low / Negative for VEGF target |
Table B — VEGF Effect, Retinal Outcome & Strength of Evidence
| Supplement | VEGF Effect | Retinal Outcome | Strength of Evidence |
|---|---|---|---|
| Vitamin D | Indirect human support; serum VEGF lowering reported in non-ophthalmic data; not firmly established in DME eye studies | Possible adjunctive benefit in central macular thickness when deficiency is corrected during bevacizumab therapy; not proven as standalone treatment | Moderate (adjunct) / Low (direct anti-VEGF) |
| Resveratrol formulations | Biologically plausible anti-VEGF activity; direct serum VEGF lowering not shown in the DME study | Greater reduction in central retinal thickness and fewer injections in one adjunctive study | Low–Moderate |
| Curcumin | Strong preclinical anti-VEGF signal; limited direct human VEGF-lowering evidence | Possible improvement in oxidative stress markers and some retinal metrics; clinical data remain early and heterogeneous | Low to Moderate |
| Omega-3 fatty acids | No consistent human proof of VEGF lowering in DR/DME | Mixed data; supportive associations, but randomized evidence for progression benefit is limited | Low |
| Lutein / Zeaxanthin | Primarily indirect; anti-VEGF claim not clinically established | May improve visual function or macular pigment support; not an established treatment for edema | Low |
| Crocin / saffron | Mechanistically plausible; direct clinical VEGF effect not established | Promising maculopathy signal in a small trial; remains investigational | Low to Moderate |
| Zinc | Negative for serum VEGF lowering in available trial | No convincing anti-VEGF retinal benefit for this question | Low / Negative for VEGF target |
Can Vitamin D Help with Diabetic Retinopathy?
Vitamin D has the strongest practical case of any supplement discussed here — but it comes with an important caveat: you need to be deficient first.
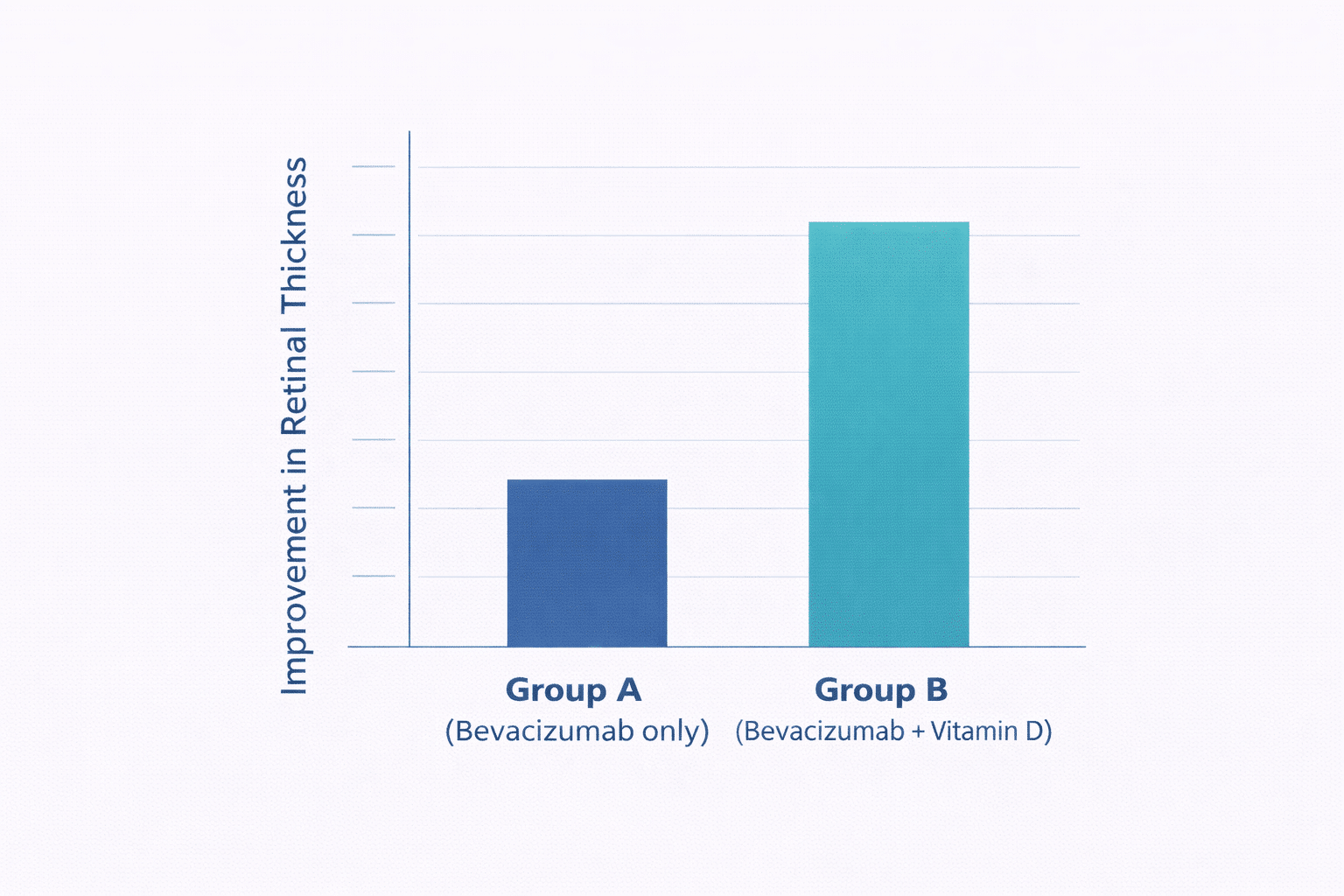
In a well-designed randomized clinical trial, patients with DME who had low vitamin D levels were treated with either bevacizumab alone or bevacizumab plus oral vitamin D supplements. Over time, those who received vitamin D had better outcomes in central macular thickness (a measure of how swollen the macula was) and visual acuity. The study does not mean vitamin D is an anti-VEGF drug — it means that correcting a deficiency may help your retina respond better to the treatment you’re already receiving.
Separately, human research in non-eye settings has shown that vitamin D supplementation can lower VEGF levels in the bloodstream among people who are deficient. That finding supports biological plausibility — but the retinal benefit remains indirect.
What this means for you: If you have diabetic retinopathy or DME, it’s reasonable to ask your doctor to check your vitamin D level (25-hydroxyvitamin D). If you’re deficient, supplementation is a sensible adjunct to standard eye care. Don’t expect it to replace your injections — but correcting a deficiency appears to be a practical supportive step.
Can Resveratrol Supplements Help Reduce DME?
Resveratrol is a plant compound found in grapes, red wine, and berries. It’s been studied for its anti-inflammatory and antioxidant effects, and basic science suggests it may reduce VEGF activity. Human evidence for diabetic eye disease is limited but more promising than that for most supplements on this list.
One small prospective study compared DME patients who received intravitreal anti-VEGF injections plus a vitamin supplement containing resveratrol with those who received injections alone. Over 12 months, the supplemented group showed a greater reduction in retinal thickness and required fewer injections. That’s an encouraging signal.
The caution: the study tested a specific combination product — not pure resveratrol alone — so the benefit cannot be attributed to resveratrol alone. The evidence base is small and has not been replicated in large trials.
What this means for you: Resveratrol-containing combinations may offer modest adjunctive benefit for some DME patients when used alongside standard treatment. This is not a proven therapy, and the effect size remains uncertain. Talk to your eye doctor before adding any supplement to your injection schedule.
What About Curcumin (Turmeric) for Diabetic Eye Disease?
Curcumin — the active compound in turmeric — is among the most-studied nutraceuticals in diabetes research, and for good reason. In laboratory models of diabetic retinal disease, curcumin consistently reduces inflammation and suppresses VEGF-related signaling pathways. The biological evidence is strong.
Human evidence is improving but remains early. A recent randomized trial of curcumin-piperine supplements in people with diabetic retinopathy showed improvements in oxidative stress markers compared with placebo. That’s meaningful, but oxidative stress markers are not the same as retinal swelling or visual acuity.
The translation problem: curcumin is poorly absorbed in most standard forms. Bioavailability varies widely by formulation, and studies use different preparations — making it hard to compare results. No large clinical trial has shown that curcumin reliably reduces retinal edema or lowers intraocular VEGF to a degree that affects treatment.
What this means for you: Curcumin is biologically interesting but not yet ready to be recommended as a treatment for diabetic eye disease. It may be worth discussing with your doctor as part of broader anti-inflammatory nutrition, but it should not replace or delay retinal therapy.
Do Omega-3 Fatty Acids Protect Your Retina?
Omega-3 fatty acids (found in fatty fish, flaxseed, and fish oil supplements) influence inflammation, endothelial function, and vascular health in ways that could theoretically benefit the diabetic retina. Observational data have suggested a protective association between higher fish consumption and better retinal outcomes.
However, randomized controlled trials in people with nonproliferative diabetic retinopathy have not consistently demonstrated that omega-3 supplements slow disease progression. The evidence is mixed.
Omega-3s are not a targeted VEGF-lowering strategy. They’re better understood as providing general cardiovascular and metabolic support — which remains relevant for people with diabetes, since controlling systemic risk factors (blood sugar, blood pressure, cholesterol) is one of the most powerful ways to slow diabetic retinopathy. Monitoring your A1c and keeping it in your target range does more for your retinal health than any supplement.
What this means for you: If your dietary intake of omega-3s is low, supplementation may be reasonable for general health — but don’t expect it to protect your eyes specifically. Focus on the fundamentals: blood sugar control, blood pressure management, and regular eye exams.
Can Lutein and Zeaxanthin Help Prevent Diabetic Eye Disease?
Lutein and zeaxanthin are carotenoids — pigments found in leafy greens and eggs — that accumulate in the macula and serve as natural antioxidants and light filters. They’re well known in the context of age-related macular degeneration (AMD), where the AREDS2 study showed benefit for certain patients.

In diabetic retinopathy, small clinical studies suggest possible improvements in visual function or macular pigment measures. However, direct human evidence that lutein and zeaxanthin lower VEGF or reduce the DME treatment burden is lacking.
These nutrients are best framed as supportive retinal nutrition — not as anti-VEGF therapy. If your diet is low in leafy greens, there’s a reasonable case for including them in a diabetes-friendly eating plan. But managing your blood sugar remains far more impactful for your eye health. Using a continuous glucose monitor to track your patterns can help you understand how your food choices affect your blood sugar throughout the day.
What Is Crocin (Saffron), and Does It Benefit the Retina?
Crocin is the active compound in saffron, and it stands out on this list because there is a placebo-controlled randomized clinical trial in people with diabetic maculopathy (a form of DME). That trial showed a clinical signal favoring crocin over placebo — more than most nutraceuticals can claim.
That said, it’s a single study with a small patient population. The evidence base is not sufficiently large or replicated to recommend crocin as a standard adjunct. It qualifies as an emerging area of interest — one worth watching in future research, but not one to act on yet based on current data.
What About Zinc? (The Answer Might Surprise You)
Zinc warrants direct attention because the human evidence here is specifically and clearly negative regarding VEGF. In a randomized controlled trial of people with diabetic retinopathy, zinc supplementation did not reduce serum VEGF compared with placebo.
Zinc plays legitimate roles in immune function and wound healing, and it’s included in some standard eye vitamins (such as AREDS2 formulations for AMD). But if the goal is to reduce VEGF or manage DME, zinc is not the right tool. This is a useful reminder that not every supplement with theoretical retinal benefits actually affects the VEGF pathway.
Important Cautions Before Starting Any Eye Health Supplement
⚠️ Talk to Your Eye Doctor First
Supplements are not regulated like medications and can interact with blood thinners, kidney disease management, and diabetes medications.
Vision-threatening DME should not be treated with supplements as a primary strategy.
Most of the studies reviewed here used supplements as add-ons to standard anti-VEGF treatment — not as replacements.
- Serum VEGF and intraocular VEGF are not the same. A blood test showing lower VEGF does not confirm that your retina is benefiting.
- Supplement studies are often small and short, and they use different formulations — making it hard to compare or apply results broadly.
- Deficiency states matter. Vitamin D supplementation showed clear benefit only in patients who were actually deficient.
- Systemic diabetes control (blood sugar, blood pressure, and cholesterol) remains the most powerful tool for slowing retinopathy progression — more so than any supplement.
- Always check for interactions with your other medications, especially blood thinners, ACE inhibitors, and immunosuppressants.
Helpful Resources & Research
For more information on managing diabetic eye disease and related topics:
- American Academy of Ophthalmology — Diabetic Retinopathy Preferred Practice Pattern, 2024
- American Academy of Ophthalmology — Intravitreal Injections Clinical Statement, 2025
- American Diabetes Association — Standards of Care in Diabetes, 2026
- Fekri et al. (2022) — Vitamin D + bevacizumab in DME. Int Ophthalmol. PMID: 35543853
- Chatziralli et al. (2022) — Resveratrol-containing supplement + anti-VEGF in DME. Eur J Ophthalmol. PMID: 34751046
- Kheirouri et al. (2019) — Zinc does not lower serum VEGF in DR. Nutr Res. PMID: 29421993
- Continuous glucose monitors — Managing your blood sugar is the most powerful way to slow diabetic retinopathy
- Diabetic retinopathy overview — Learn more about how diabetes affects your eyes
Frequently Asked Questions About Supplements for Diabetic Retinopathy
Can supplements replace anti-VEGF injections in treating diabetic macular edema?
No. Anti-VEGF injections work directly inside the eye to block the protein that causes leakage and swelling. No supplement has been shown to do this reliably. Supplements may play a supportive role for some patients, but they cannot replace proven treatments for center-involved DME.
Which supplement has the strongest evidence for diabetic eye disease?
Vitamin D repletion has the strongest practical clinical support — specifically in patients who are deficient and already receiving anti-VEGF treatment. It should be considered an adjunct, not a primary therapy. Resveratrol-containing combination supplements also have limited but somewhat promising data.
Does zinc help with VEGF and with diabetic retinopathy?
No — in fact, a randomized controlled trial found that zinc supplementation did not reduce serum VEGF levels in people with diabetic retinopathy. Zinc is not a good choice if the goal is to specifically reduce VEGF.
Is curcumin (turmeric) beneficial for diabetic retinopathy?
Curcumin has strong evidence in the lab but limited clinical proof in humans for retinal VEGF suppression. Early trials show improvements in oxidative stress markers, but these haven’t translated into proven benefits for retinal edema or vision. It may be considered a biologically plausible adjunct, though current evidence is limited.
What are the best vitamins for overall diabetic eye health?
The most commonly recommended supplements are vitamin D (if deficient), lutein/zeaxanthin (for antioxidant support), and omega-3 fatty acids (for general metabolic and vascular health). Always discuss starting supplements with your doctor, especially if you’re on diabetes medications or blood thinners.
Can I take eye supplements while receiving anti-VEGF injections?
Some patients take supplements alongside injections — particularly vitamin D or resveratrol-containing products — but this should always be coordinated with your retina specialist. Your doctor can check for interactions and monitor whether the combination is helpful in your specific case.
How does blood sugar control influence diabetic retinopathy?
Managing your blood sugar is the most effective way to slow the progression of diabetic retinopathy — far more effective than any supplement. The A1c test (your average blood sugar over 2–3 months) is the key metric. Every 1% reduction in A1c is associated with a meaningful decrease in the risk of retinal complications. Aim for the target range your doctor recommends, typically below 7–7.5% for most adults.
What is VEGF, and why does it matter in diabetes?
VEGF (vascular endothelial growth factor) is a protein that signals the body to form new blood vessels. In diabetic eye disease, persistently high blood sugar damages retinal blood vessels, triggering excessive VEGF production. This results in leaky, abnormal vessels and fluid buildup (macular edema), which can blur or damage vision. Anti-VEGF injections block this process inside the eye.
Is saffron (crocin) effective for diabetic macular edema?
Crocin, the active compound in saffron, has one small randomized, placebo-controlled trial showing a clinical benefit for diabetic maculopathy. This is more human evidence than most nutraceuticals have, but the study is small and has not been replicated. Crocin should be considered investigational at this stage.
Are omega-3 supplements proven to prevent the progression of diabetic retinopathy?
Not definitively. While observational studies suggest that higher fish intake may be protective, randomized controlled trials of omega-3 supplements for nonproliferative diabetic retinopathy have yielded mixed results. Omega-3s are better suited for general metabolic support than for targeted retinopathy treatment.
Last Updated on June 2, 2026